A 38-year old male patient presented with complaints of blurred vision and decreased visual acuity in the left eye. The patient had no systemic problems and did not report any chronic drug use. The patient reported previous similar blurred vision complaints The best corrected visual acuity (BCVA) was 20/20 in the right eye and 20/100 in the left eye. Anterior segment examinations of both eyes were unremarkable.
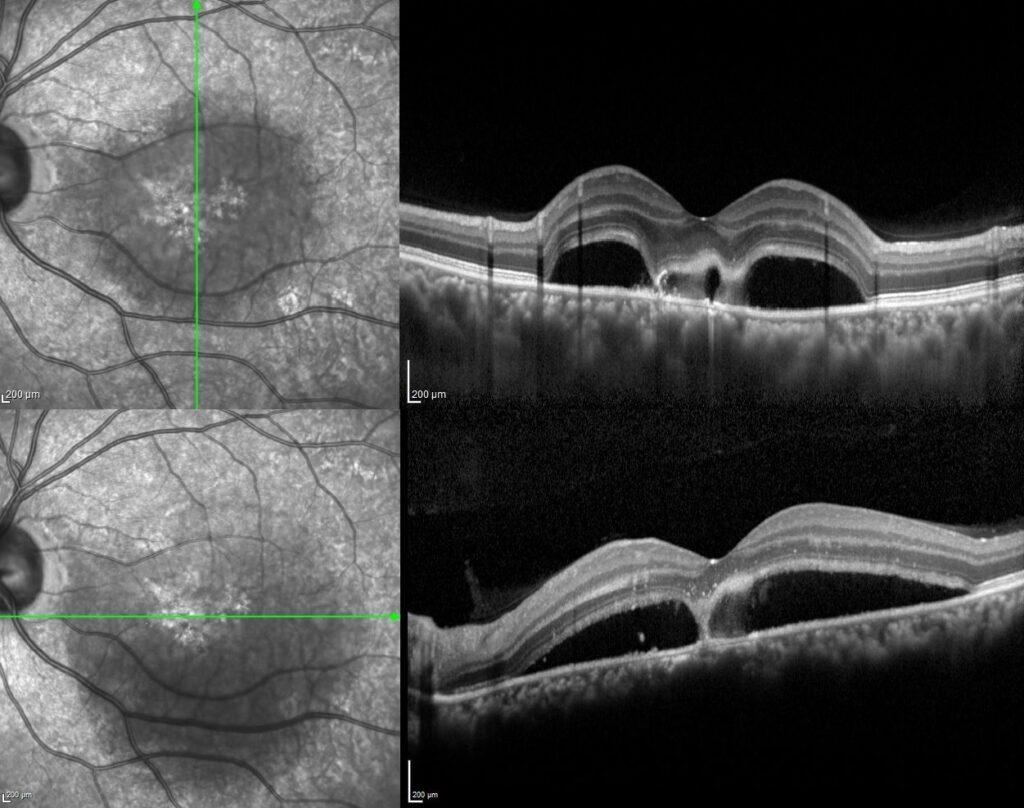
Dilated fundus examination demonstrated while the posterior segment of the right eye was completely normal, in the left eye there was a well-defined diffuse serous retinal detachment, a yellowish subretinal fibrinous material accumulation adjacent to the fovea, and a darker spot within the yellowish fibrin.

In the early phase of the fluorescein angiography in the left eye, the point of leakage in the RPE was seen as hyperfluorescence, and atrophic areas as a result of previous attacks were hyperfluorescent. In the late phase, the hyperfluorescence at the active leakage point did not change and the serous retinal detachment area became more prominent.

The spectral domain OCT scan passing through the area of fibrinous material revealed serous detachment, hyper-reflective fibrinous material accumulation extending from the RPE to the subretinal area within the detachment area, and two vacuolar structures visible as hyporeflective spaces amid the hyper-reflective fibrin.
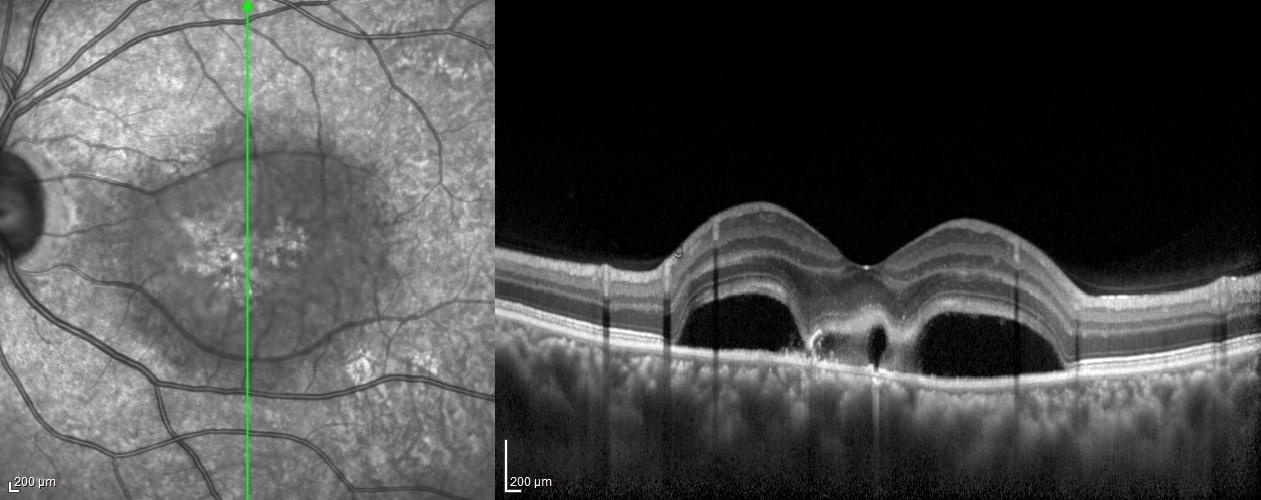
Optic coherence tomography has an important role in the diagnosis and follow-up of central serous chorioretinopathy. Several OCT studies have demonstrated hyper-reflectivity in the subretinal space corresponding to the fibrin material and have also demonstrated dipping of the neurosensory retina at the site of fibrin formation. Sometimes, this fibrin accumulation has hyporeflective areas and has been named the vacuole sign. It was reported that the presence of a hyporeflective vacuole amid the hyper-reflective fibrin adjacent to RPE defects probably indicates the site of constant fluid egress. It was also emphasized that the vacuol sign could be an important indicator of disease activity, especially in cases where angiography is not possible.
Credit: Kemal Tekin, M.D., from Ulucanlar Eye Training and Research Hospital
Instagram accounts: @retina.academy and @dr.kemaltekin
