Central retinal vein occlusion (CRVO) may present as non-ischemic or ischemic CRVO. This distinction is clinically important because ischemic CRVO has a higher risk of severe visual loss, extensive retinal nonperfusion, iris neovascularization, and neovascular glaucoma.
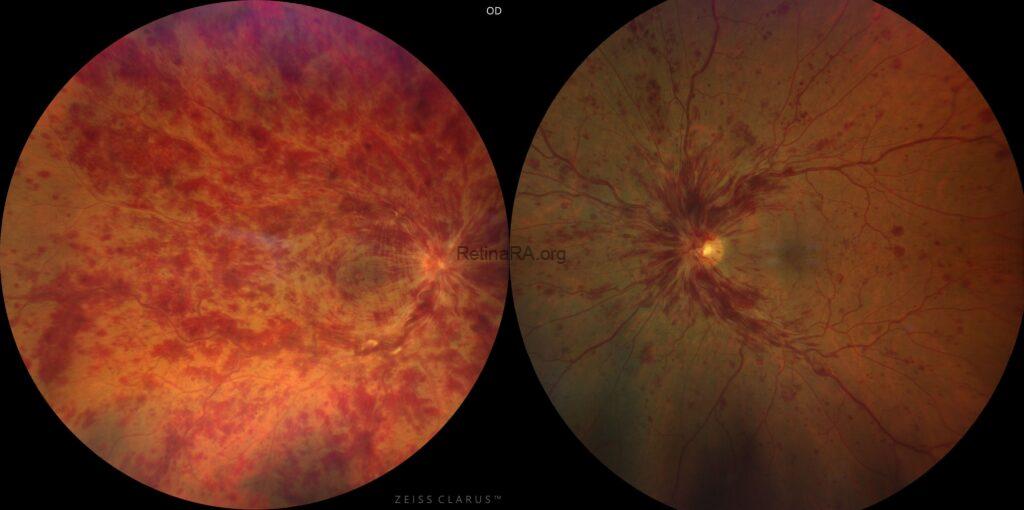
Case 1 — Ischemic CRVO
70-year-old female, hypertension (+)
VA: 20/400
RAPD: Positive
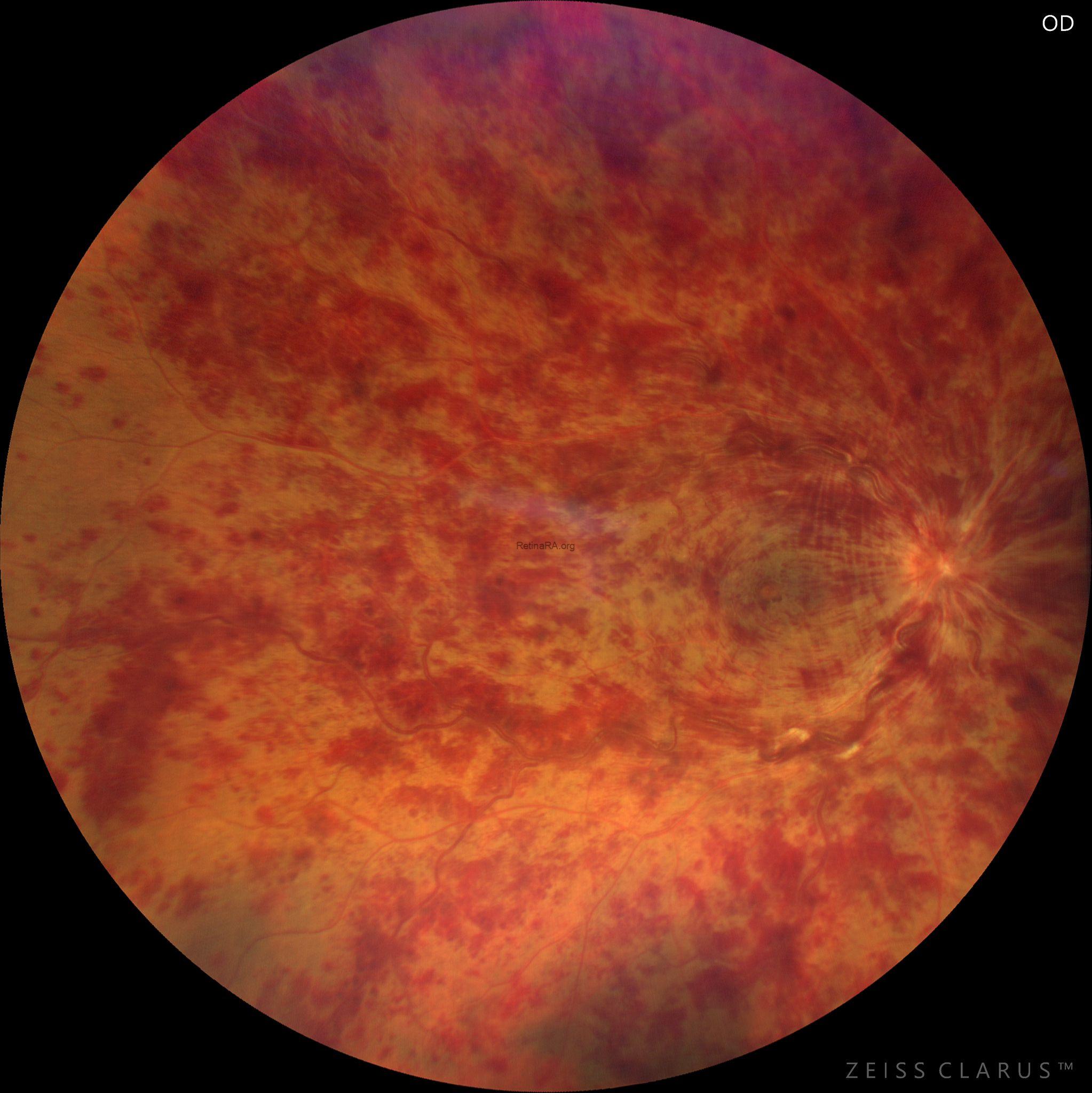 Fundus findings show extensive deep retinal hemorrhages, severe venous tortuosity and engorgement, cotton-wool spots, macular edema, and severe optic disc edema.
Fundus findings show extensive deep retinal hemorrhages, severe venous tortuosity and engorgement, cotton-wool spots, macular edema, and severe optic disc edema.
Key clues:
Severe visual loss, positive RAPD, extensive hemorrhages, cotton-wool spots, severe venous tortuosity, marked disc edema.
Case 2 — Non-Ischemic CRVO
65-year-old female, hypertension (+)
VA: 20/70
RAPD: Negative
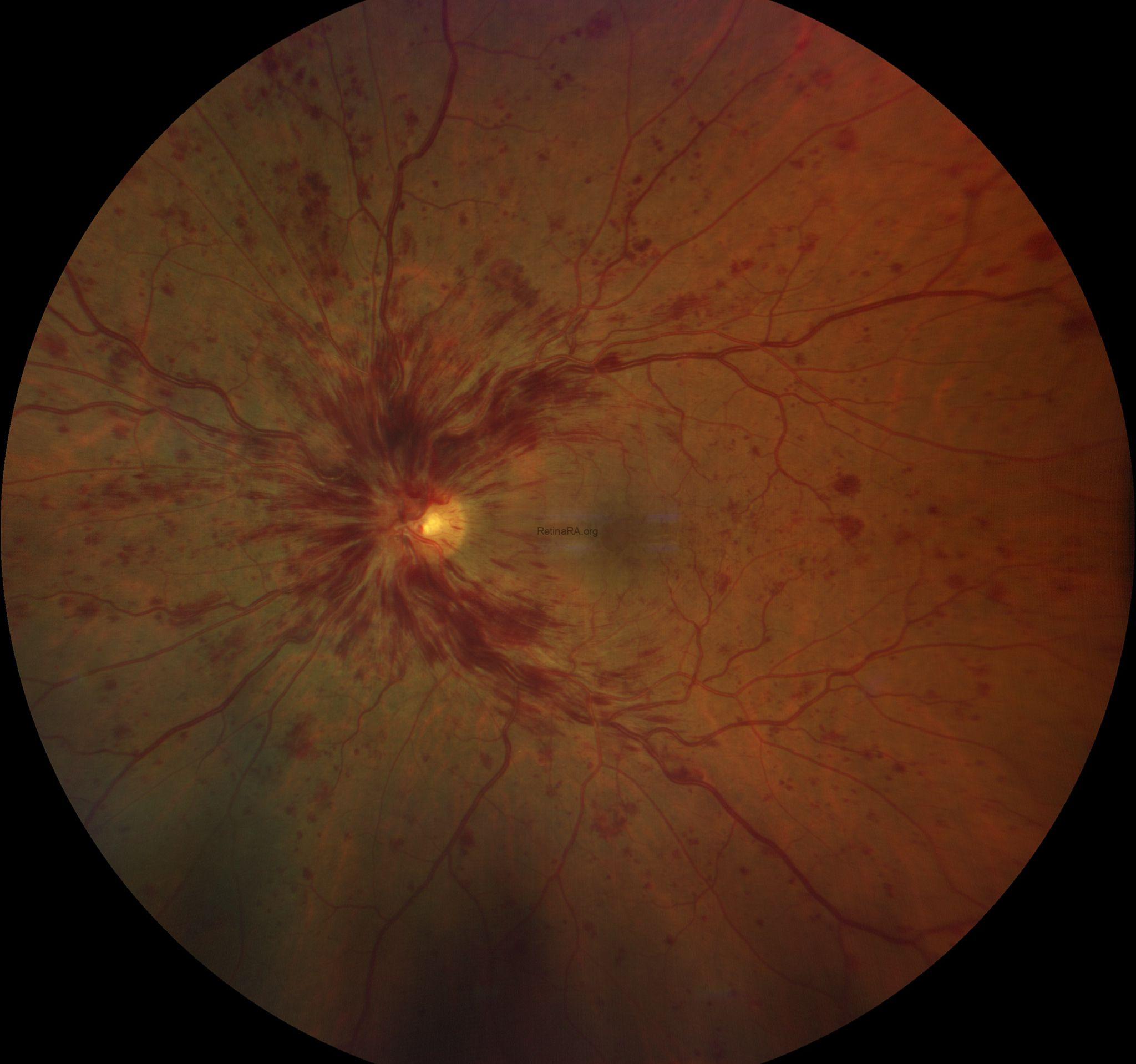
Fundus findings show four-quadrant dot/blot and flame-shaped hemorrhages with mild optic disc edema.
Key clues:
Relatively good visual acuity, negative RAPD, mild disc edema, less extensive hemorrhagic changes.
Clinical differentiation between non-ischemic and ischemic CRVO is based on both functional and fundus findings. In non-ischemic CRVO, visual acuity is usually relatively preserved, RAPD is absent or mild, retinal hemorrhages are mild to moderate, cotton-wool spots are few or absent, optic disc edema is mild to moderate, and venous tortuosity is less pronounced. In contrast, ischemic CRVO typically presents with severely reduced visual acuity, a definite RAPD, extensive or confluent retinal hemorrhages, frequent cotton-wool spots, marked optic disc edema, and severe venous tortuosity and engorgement. The risk of ocular neovascularization is substantially higher in ischemic CRVO.
Severe visual loss and a positive RAPD are among the most important clinical clues suggesting ischemic CRVO. Fundus findings support the diagnosis, but fluorescein angiography or widefield imaging is required to confirm the extent of retinal nonperfusion.
Credit: Kemal Tekin, M.D., from Ulucanlar Eye Training and Research Hospital
Instagram accounts: @retina.academy and @dr.kemaltekin
