A 34-year-old male presented with decreased vision in the right eye. Symptoms began 2 years ago, and follow-up examinations showed a partial but incomplete resolution of subretinal fluid. Best-corrected visual acuity was 20/30 in the right eye and 20/20 in the left eye, with intraocular pressures within normal limits bilaterally. Anterior segment examination was unremarkable, and fundus evaluation revealed findings consistent with chronic central serous chorioretinopathy in the right eye, while the left eye appeared normal.

Color fundus photography of the right eye, there is a large serous retinal detachment extending inferiorly, with a clear gravitational track of subretinal fluid descending from the fovea towards the inferior retina. The optic disc appears normal, and the retinal vasculature is within normal caliber.

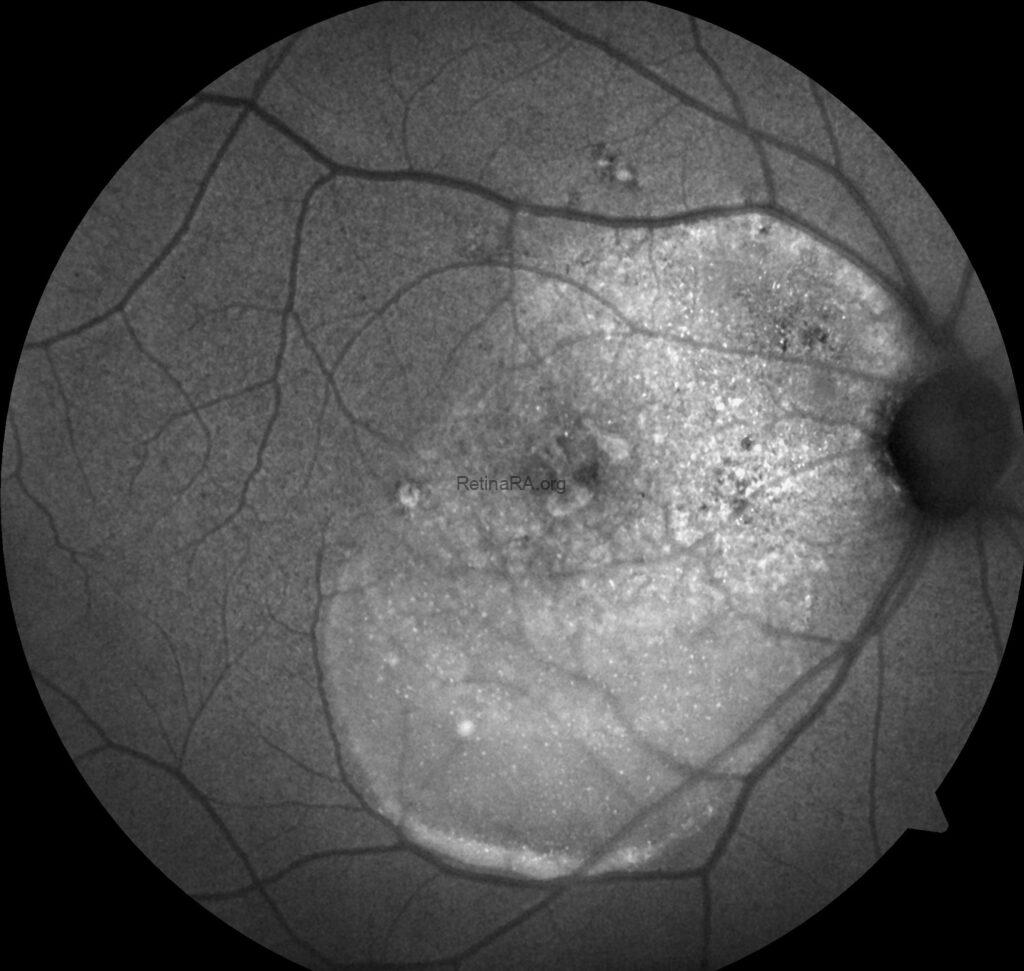
Fundus autofluorescence (FAF) imaging of the right eye demonstrates a large area of diffuse hyperautofluorescence extending from the fovea towards the inferior retina, consistent with the gravitational tract of chronic subretinal fluid. Patchy hypoautofluorescent spots within the area correspond to retinal pigment epithelium (RPE) atrophy. Multiple punctate hyperautofluorescent foci are scattered within and around the detachment zone, likely reflecting areas of photoreceptor and RPE stress. The optic disc shows normal autofluorescence.

Spectral-domain optical coherence tomography (SD-OCT) of the right eye demonstrates a dome-shaped serous retinal detachment involving the fovea, with persistent subretinal fluid. A shallow, irregular pigment epithelial detachment (PED) is noted beneath the neurosensory retina. The photoreceptor layer shows elongation and focal disruption of the ellipsoid zone, consistent with chronic photoreceptor damage. Overlying the subretinal fluid, alternating hyperreflective and hyporeflective bands are present, corresponding to the characteristic “barcode sign” due to RPE hyperplasi. The choroid appears markedly thickened, with dilated outer choroidal vessels (pachyvessels) consistent with pachychoroid phenotype.

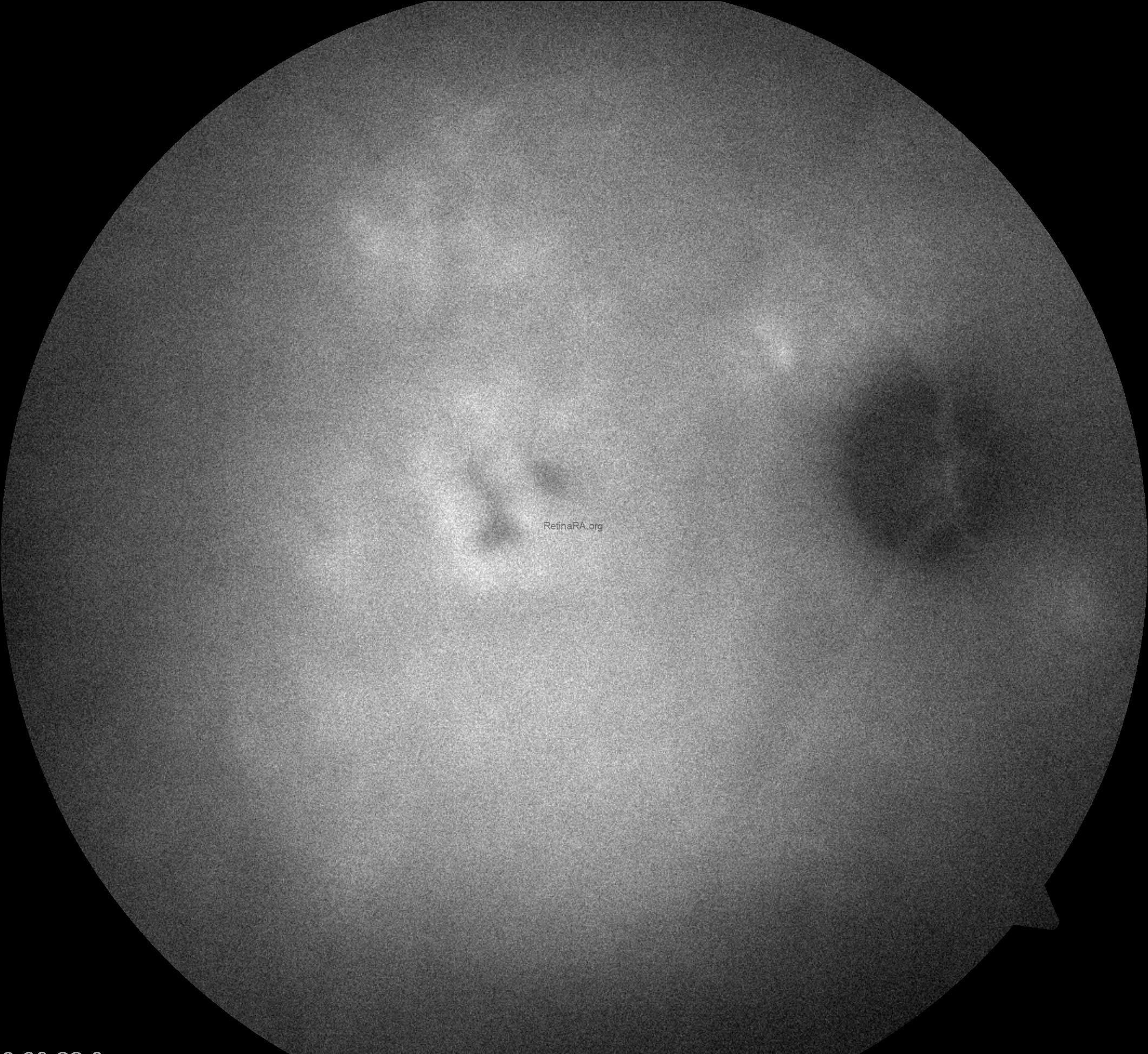
Indocyanine green angiography (ICGA) of the right eye revealed early-phase choroidal hyperpermeability with markedly dilated outer choroidal vessels (pachyvessels), consistent with the pachychoroid phenotype. During the mid-early phase, there was persistent choroidal filling and diffuse hyperfluorescence extending beyond the macular region, indicating widespread choroidal vascular leakage. In the mid-late phase, a focal hyperfluorescent leakage area became more evident at the macula, corresponding to the clinically observed site of subretinal fluid accumulation. Late-phase images demonstrated persistent hyperfluorescence with staining of the retinal pigment epithelium (RPE) alterations along the inferior gravitational tract, without evidence of choroidal neovascularization. These findings are characteristic of chronic central serous chorioretinopathy, reflecting sustained choroidal hyperpermeability and RPE damage.

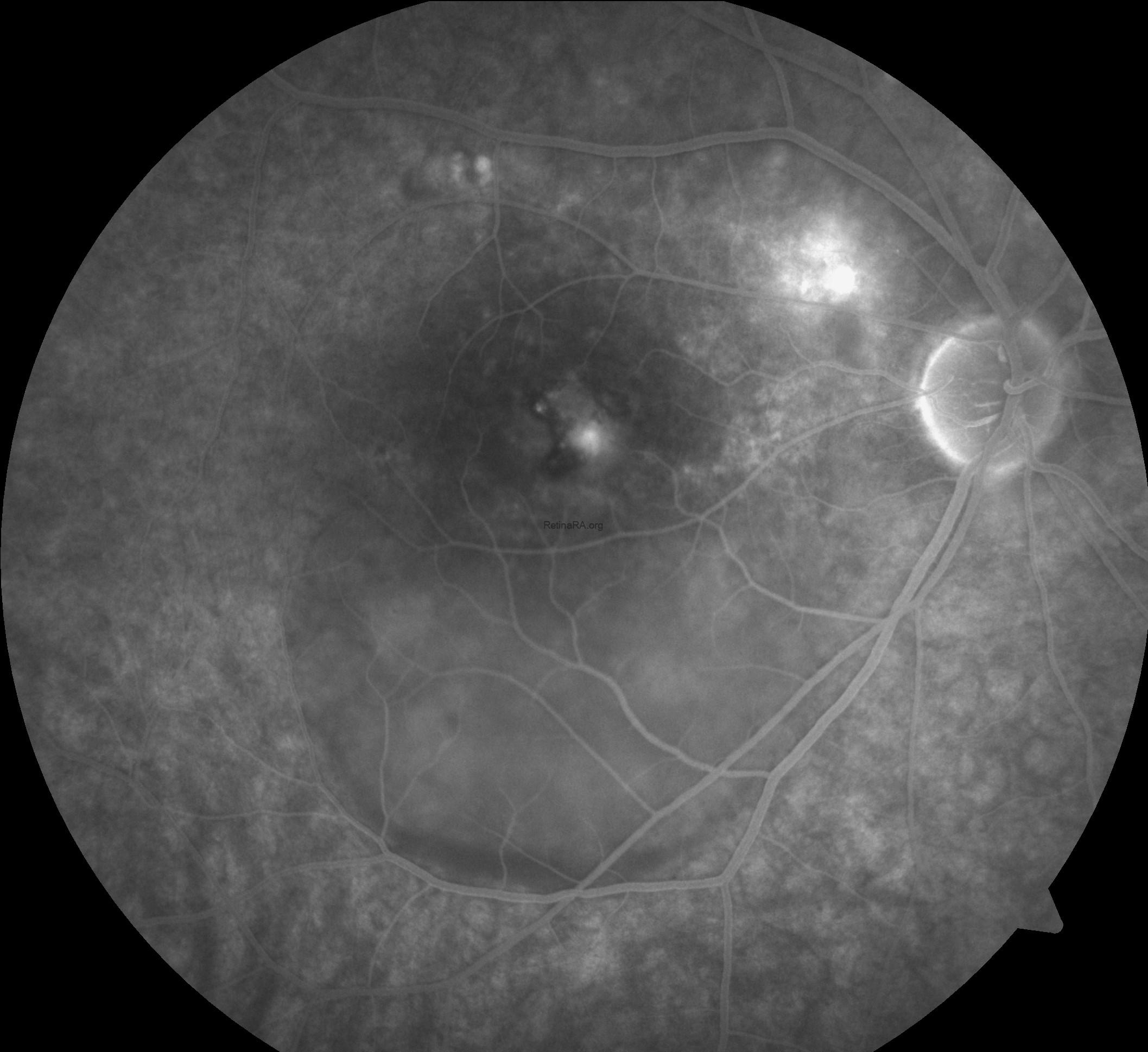
Fluorescein angiography (FFA) of the right eye shows multiple areas of early hyperfluorescence in the macula representing RPE window defects, with a discrete focal leak near the fovea that enlarges over time in an ink-blot pattern. As the study progresses, dye accumulates in the subretinal space with evident pooling and a descending gravitational tract toward the inferior posterior pole, matching the clinically visible detachment. Late frames demonstrate persistent pooling with diffuse staining of chronically altered RPE and the margins of shallow, irregular PEDs, while the optic disc remains non-leaky. There is no lacy capillary network, stippled hyperfluorescence with late leakage, or other features suggestive of choroidal neovascularization, and no vasculitis or peripheral ischemia. Overall, the angiographic pattern is consistent with chronic central serous chorioretinopathy and correlates with OCT-documented subretinal fluid and PED.

Enface OCT ( outer retina slab) of the right eye in , attenuation of the outer retinal signal was observed overlying the detachment, corresponding to chronic photoreceptor disruption. The perifoveal capillary plexuses appeared intact without microvascular abnormalities, confirming the absence of ischemic changes at the retinal level.
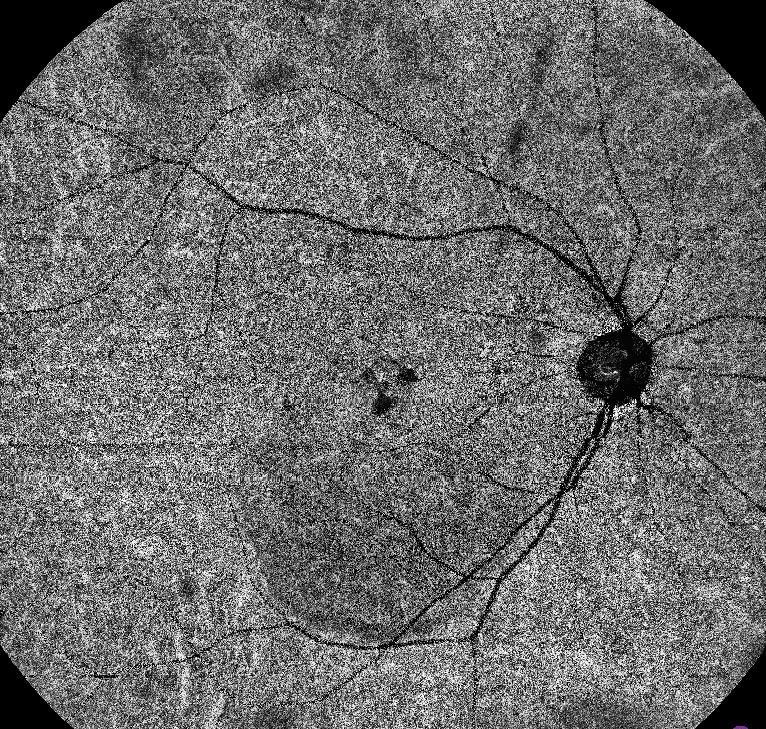
15×15 mm scan of the choriocapillaris slab reveals multiple confluent flow voids in the subfoveal region extending inferiorly along the gravitational tract, corresponding to the area of chronic subretinal fluid. These flow voids are associated with mottled signal loss in surrounding regions, reflecting chronic choriocapillaris hypoperfusion and overlying RPE alterations. The peripapillary choriocapillaris appears relatively preserved, with no evidence of abnormal high-flow lesions suggestive of macular neovascularization. The overall pattern is consistent with chronic central serous chorioretinopathy, characterized by localized and diffuse choriocapillaris impairment secondary to long-standing choroidal hyperpermeability.

15×15 mm scan of the avascular slab demonstrates a well-demarcated hyporeflective area in the subfoveal region corresponding to persistent subretinal fluid. The outer retina shows attenuation of flow signal overlying the detachment, consistent with chronic photoreceptor layer disruption. Perifoveal and parafoveal regions display preserved capillary-free zones with intact superficial and deep vascular plexus margins. No abnormal high-flow signal suggestive of macular neovascularization is identified. The overall pattern is in keeping with chronic central serous chorioretinopathy, with secondary signal loss in the avascular layer due to neurosensory retinal elevation.
Chronic central serous chorioretinopathy (CSC) is characterized by persistent subretinal fluid, photoreceptor damage, thickened choroid, and retinal pigment epithelium (RPE) dysfunction. Multimodal imaging—including color fundus photography, fundus autofluorescence (FAF), optical coherence tomography (OCT), fluorescein angiography (FFA), indocyanine green angiography (ICGA), and OCT angiography (OCTA)—plays a critical role in diagnosis and differentiation from other retinal pathologies .
Credit: M. Giray Ersoz, MD, FEBO, Retina Specialist
Memorial Bahçelievler Hospital, Department of Ophthalmology, Istanbul, Turkey
Arel University School of Medicine, Department of Ophthalmology, Istanbul, Turkey
Instagram accounts: @retina.review and @retina.dr.girayersoz
Website: www.girayersoz.com.tr
and Sepideh Lotfi, MD
Biruni University School of Medicine, Department of Ophthalmology, Istanbul, Turkey
Instagram accounts: @sepidls
