A 27-year-old woman presented with a 2–3-week history of significant visual loss in her left eye. Her ocular history was notable for bilateral LASIK surgery performed six years earlier for -5.00 diopters of myopia.
At presentation, best-corrected visual acuity was 20/20 in the right eye, while the left eye had a visual acuity of counting fingers at 1 meter. Anterior segment examination was unremarkable except for previous LASIK surgery.
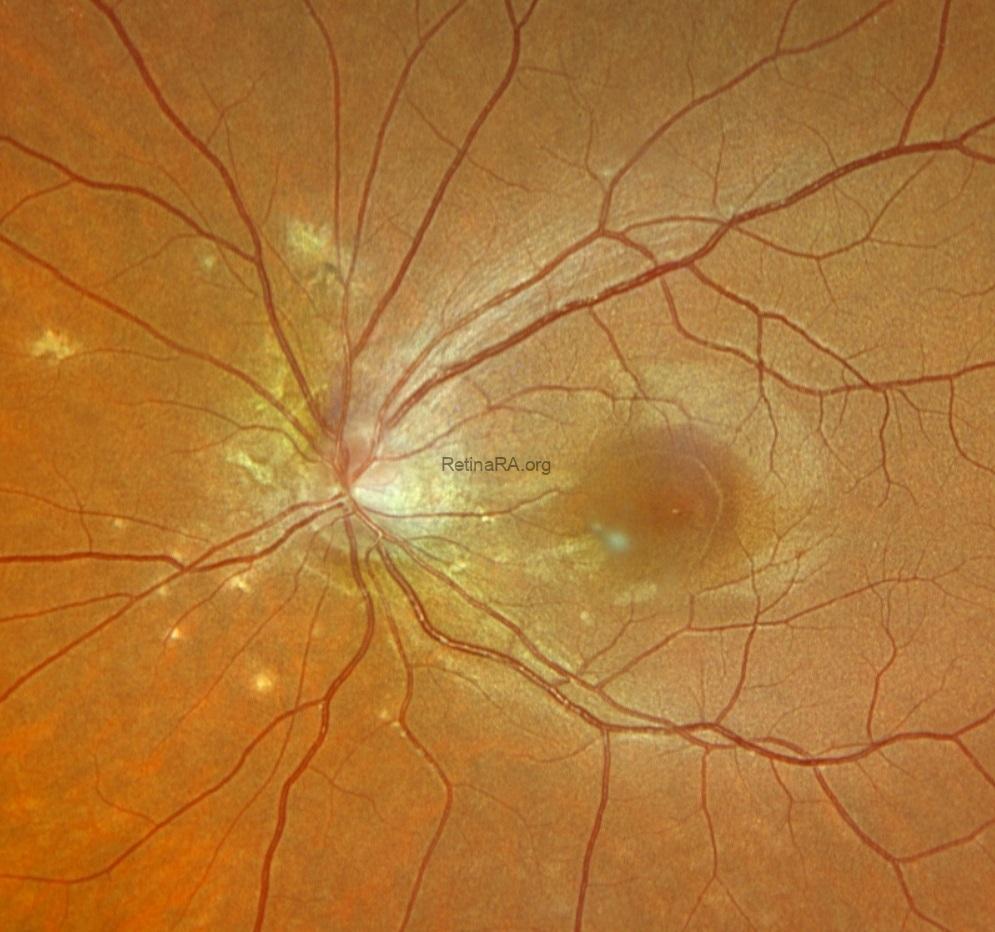
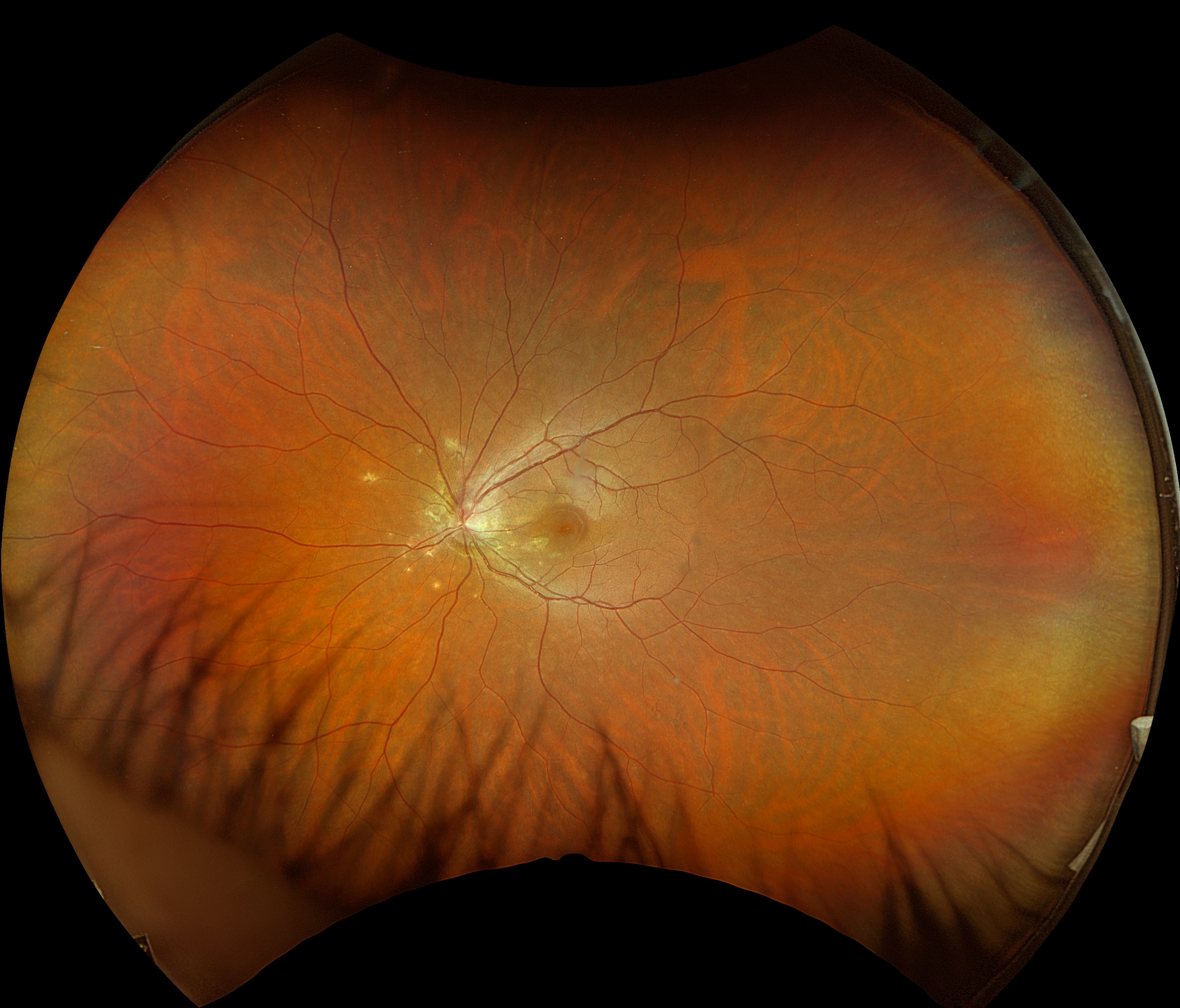
Fundus examination of the left eye revealed multiple small yellow-white lesions distributed throughout the peripapillary region and posterior pole. No vitreous inflammation was observed. Ultra-widefield imaging demonstrated no peripheral retinal or choroidal lesions. The right eye was normal.
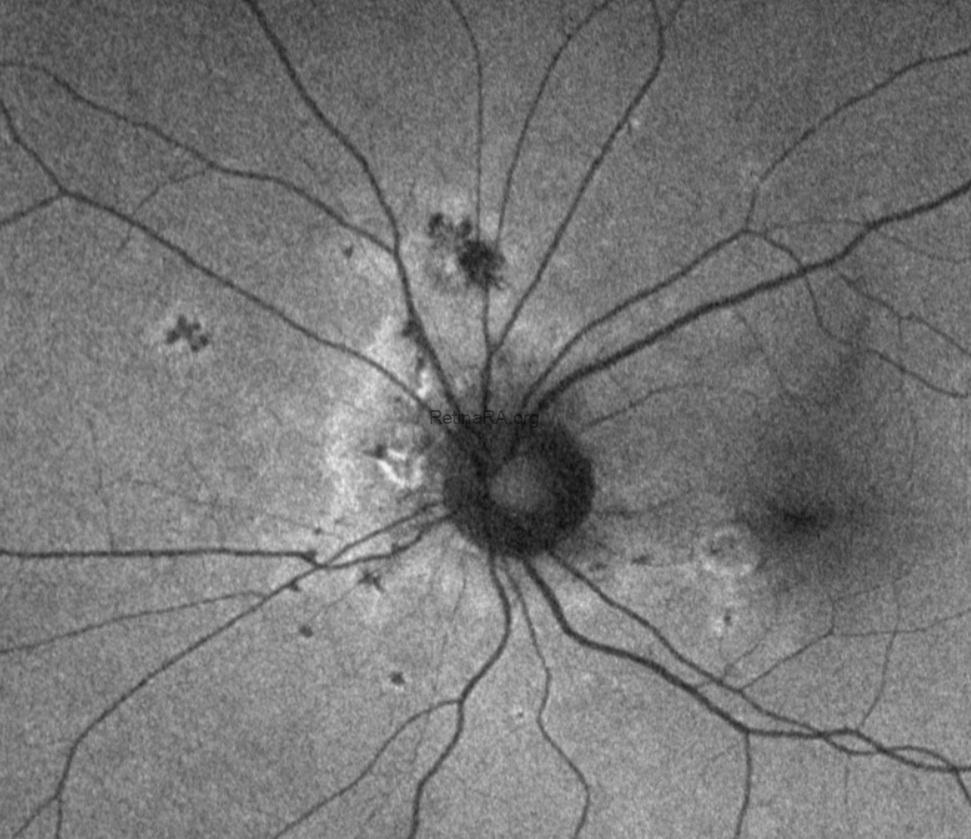
 Fundus autofluorescence (FAF) image
Fundus autofluorescence (FAF) image
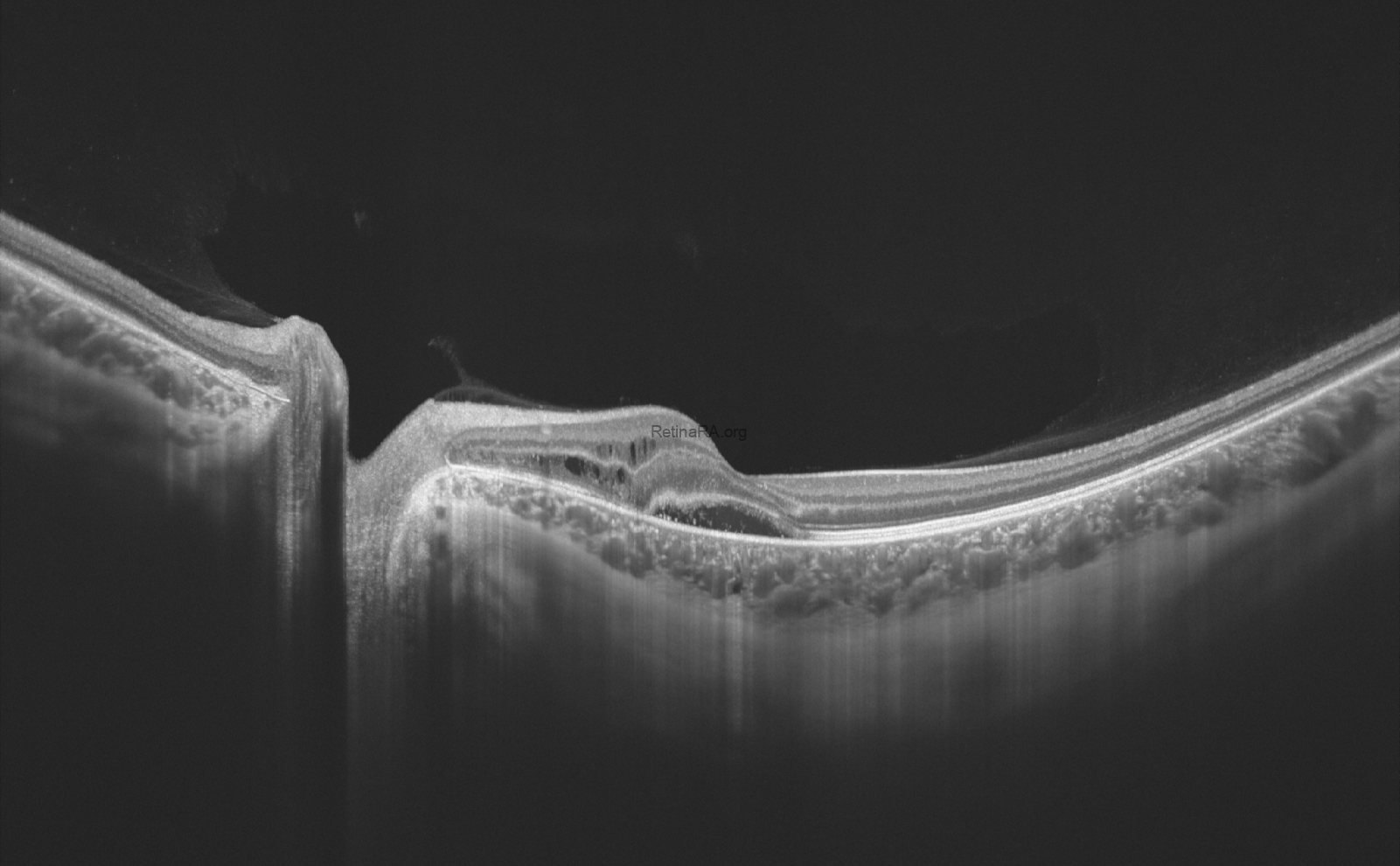
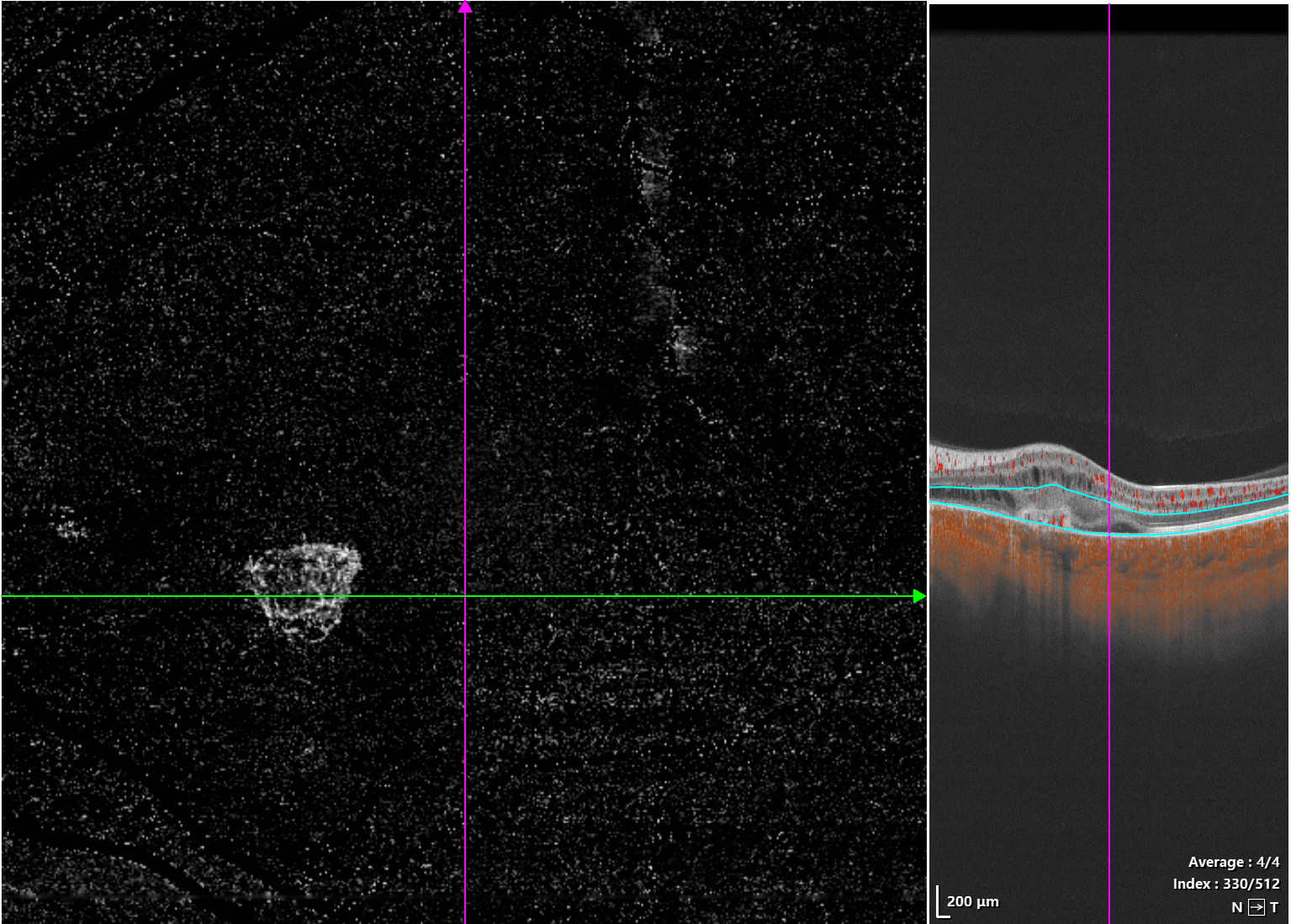
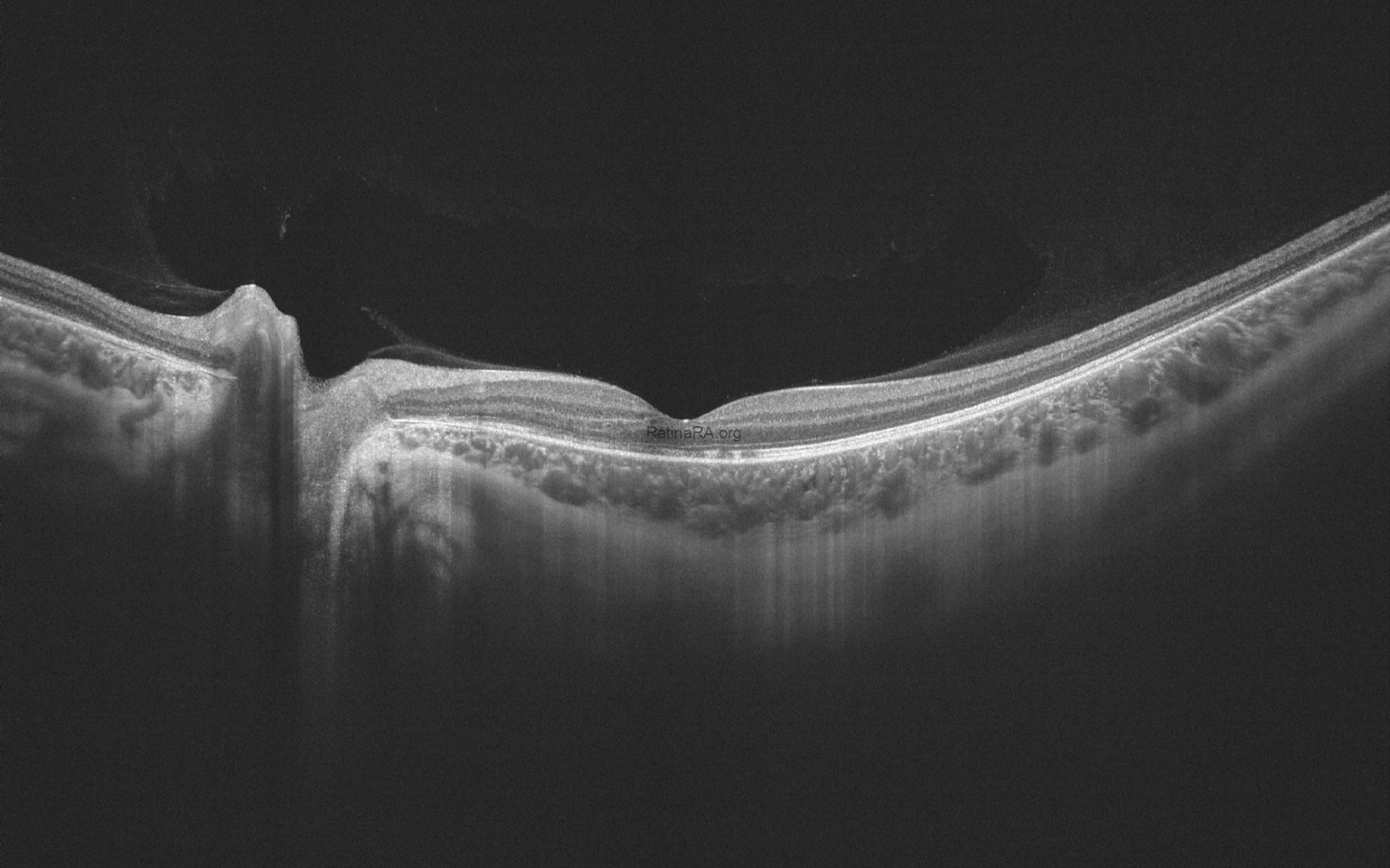
 Optical coherence tomography (OCT) showed both subretinal and intraretinal fluid located in the papillomacular region between the optic disc and the fovea.
Optical coherence tomography (OCT) showed both subretinal and intraretinal fluid located in the papillomacular region between the optic disc and the fovea.
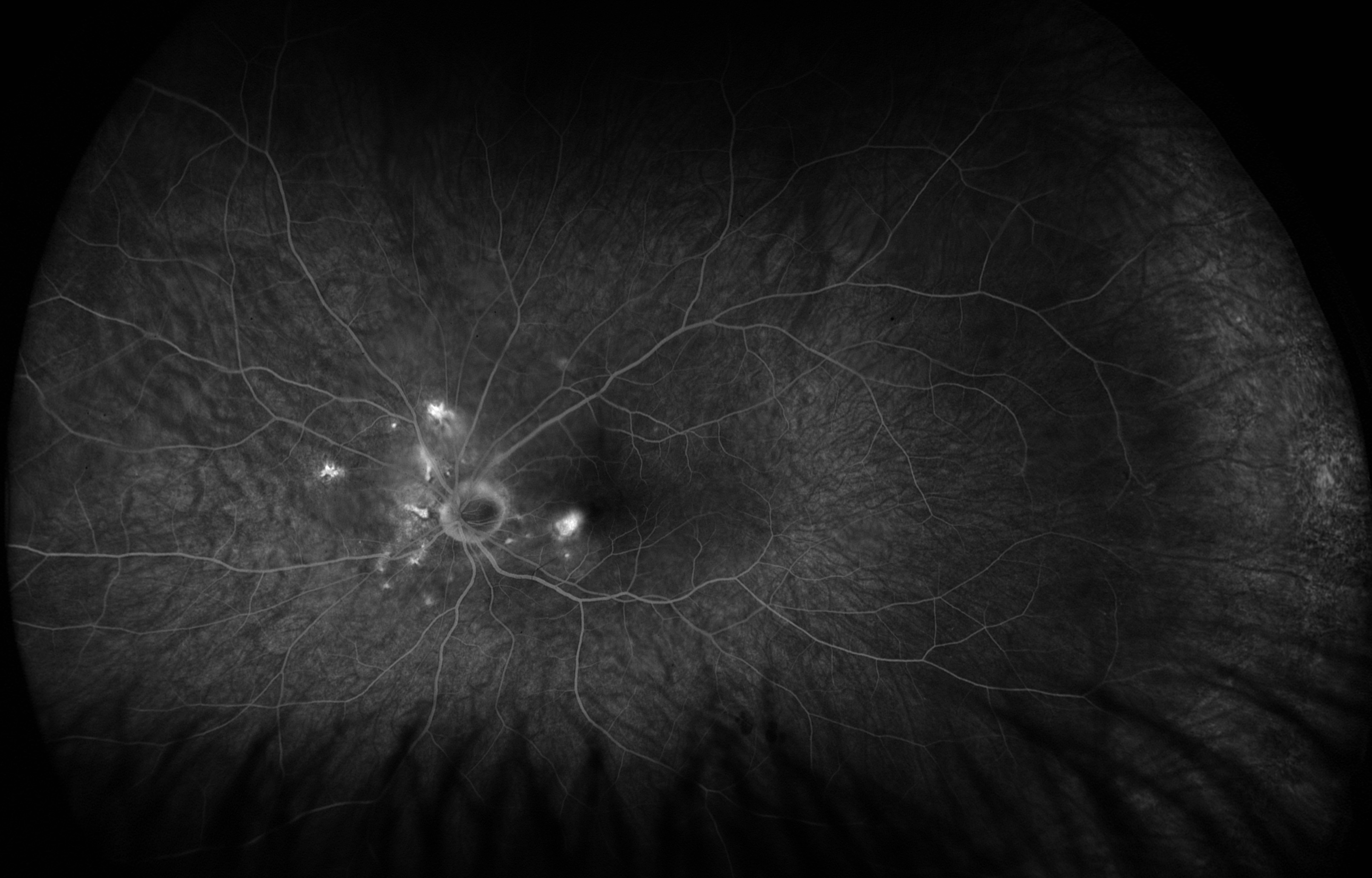
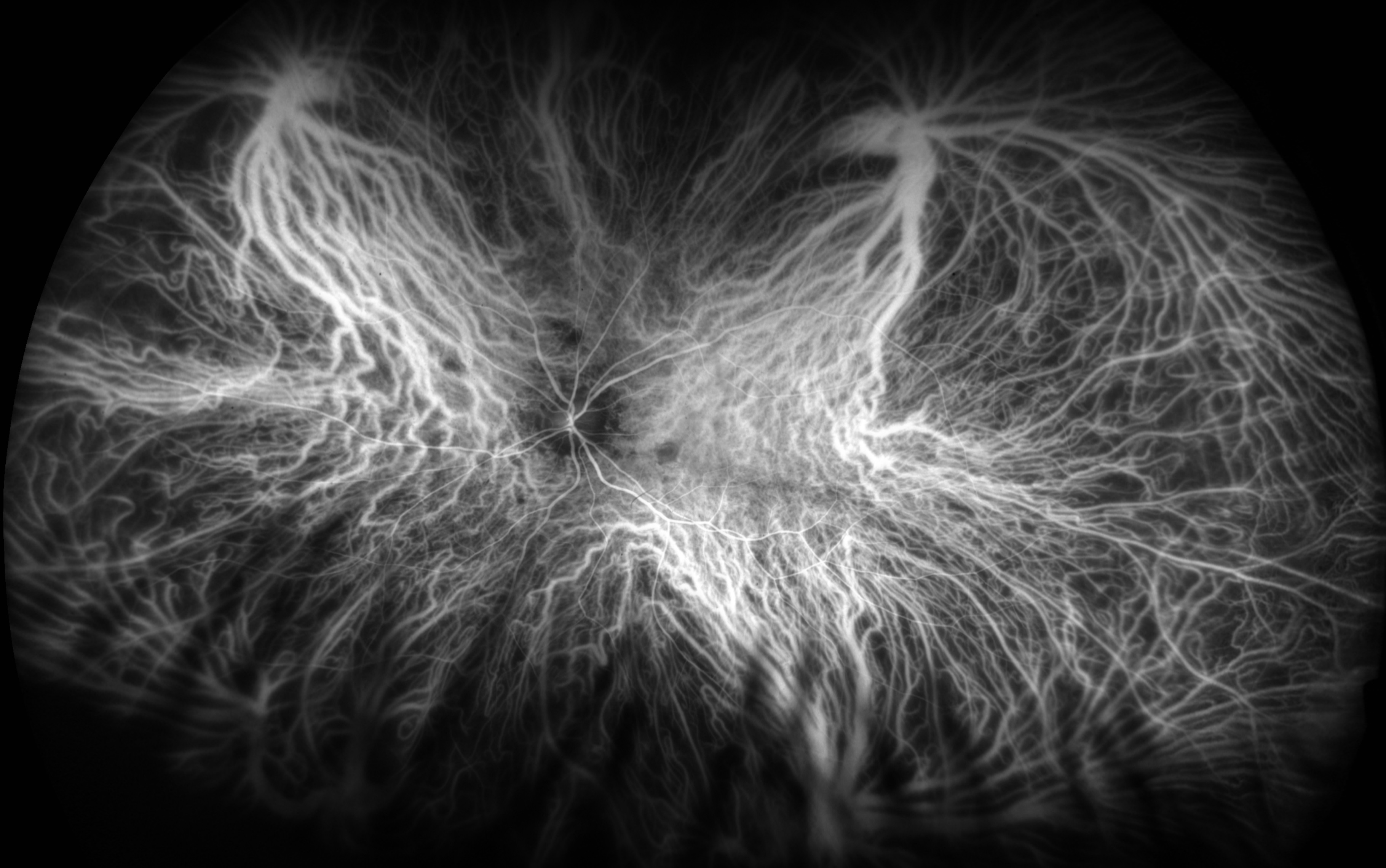
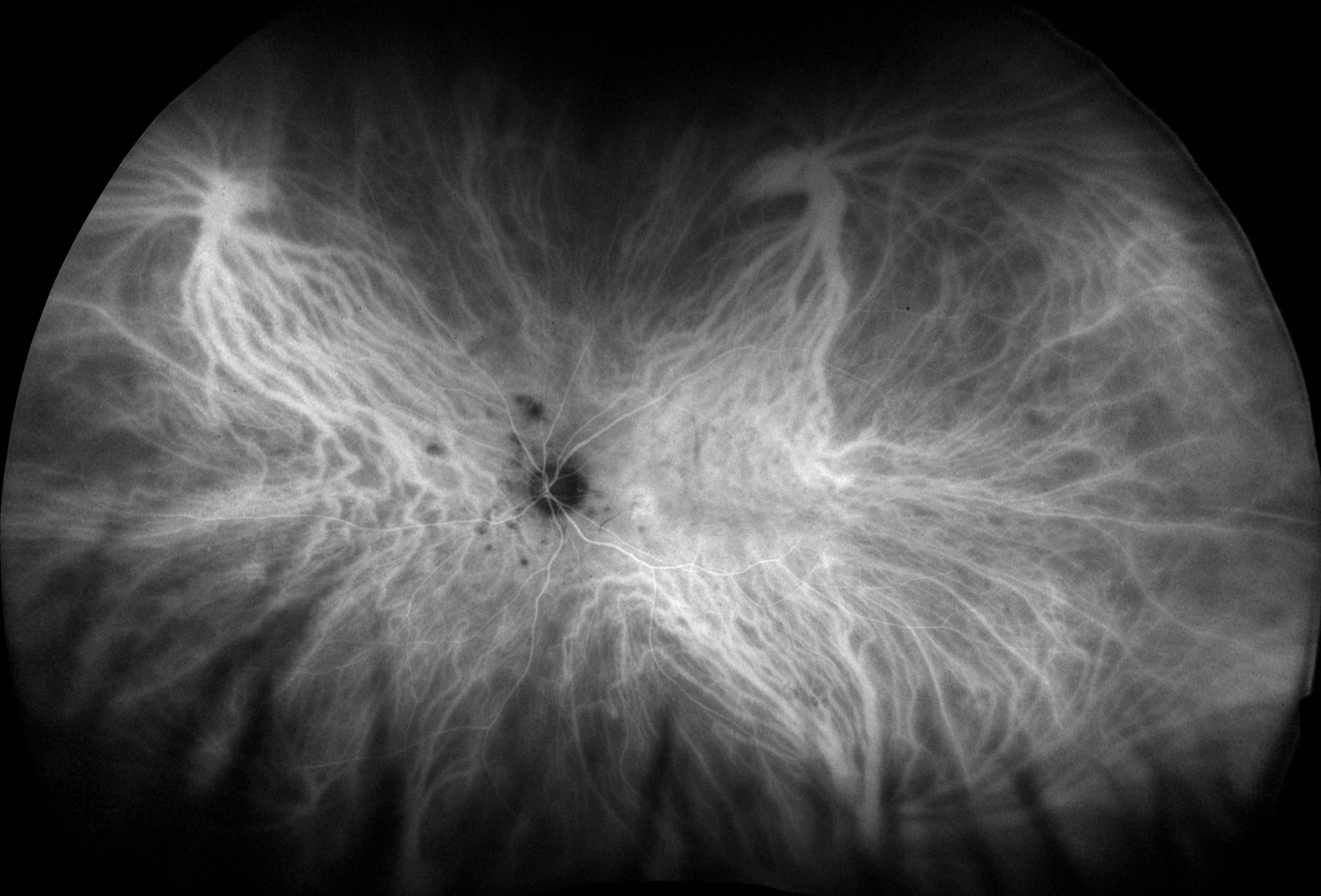
 Fluorescein angiography demonstrated mild hyperfluorescence of the lesions in the early phases, followed by progressive staining in the late phases. Ultra-widefield fluorescein angiography showed no evidence of peripheral lesions, retinal vasculitis, or other inflammatory vascular abnormalities.
Fluorescein angiography demonstrated mild hyperfluorescence of the lesions in the early phases, followed by progressive staining in the late phases. Ultra-widefield fluorescein angiography showed no evidence of peripheral lesions, retinal vasculitis, or other inflammatory vascular abnormalities.
Early-phase FA
 Late-phase FA
Late-phase FA
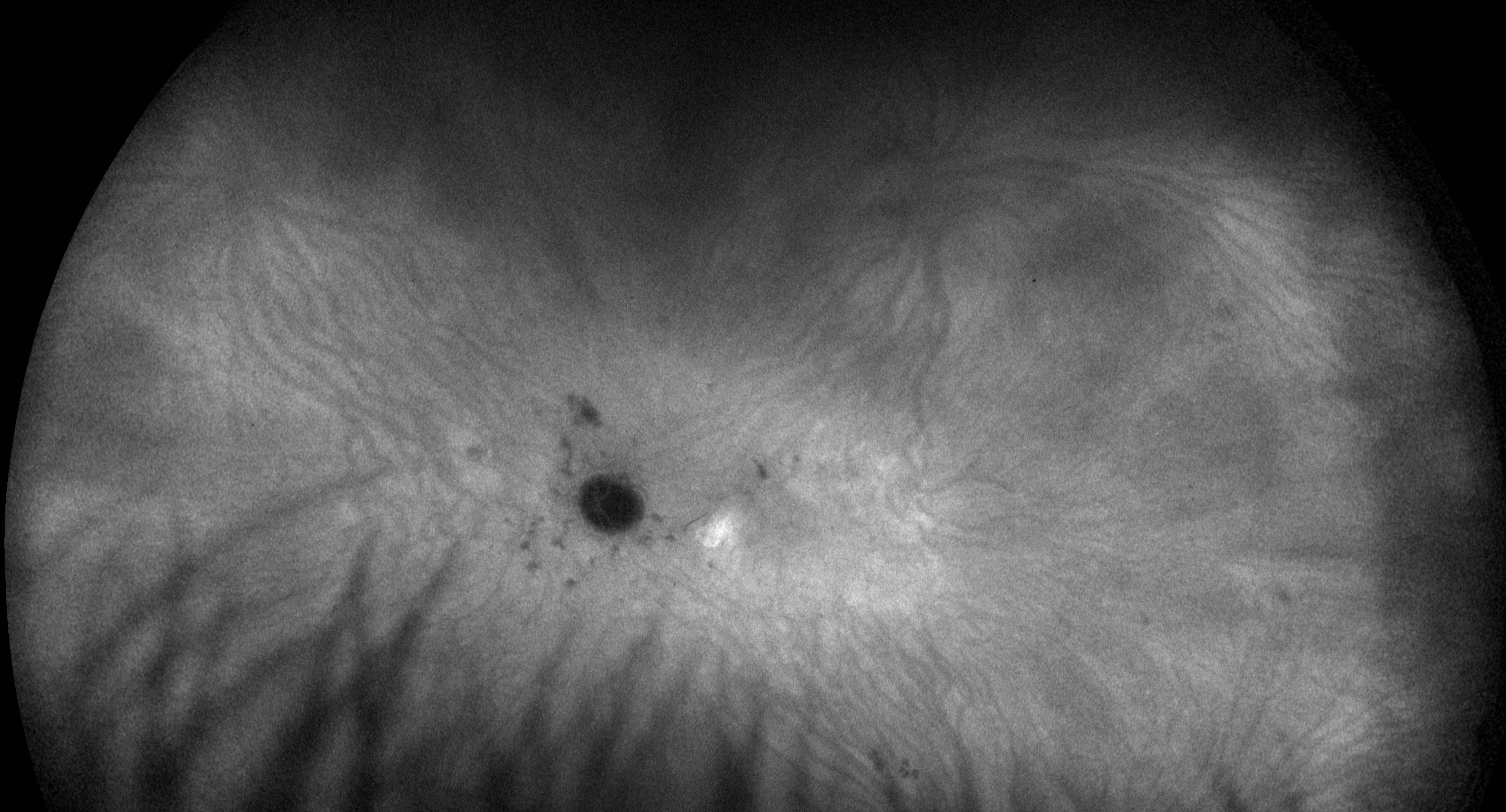
 Indocyanine green angiography revealed corresponding early and late hypofluorescent lesions.
Indocyanine green angiography revealed corresponding early and late hypofluorescent lesions.
Early-phase ICGA
 Mid-phase ICGA
Mid-phase ICGA
 Late-phase ICGA
Late-phase ICGA
 FA, ICGA, and OCTA also demonstrated a choroidal neovascular membrane located in the papillomacular region between the optic disc and the fovea, accounting for the retinal fluid and severe visual loss.
FA, ICGA, and OCTA also demonstrated a choroidal neovascular membrane located in the papillomacular region between the optic disc and the fovea, accounting for the retinal fluid and severe visual loss.
 Based on the patient’s demographic characteristics, clinical examination, multimodal imaging findings, absence of vitritis, and the presence of choroidal neovascularization, a diagnosis of punctate inner choroidopathy (PIC) was established.
Based on the patient’s demographic characteristics, clinical examination, multimodal imaging findings, absence of vitritis, and the presence of choroidal neovascularization, a diagnosis of punctate inner choroidopathy (PIC) was established.
Treatment was initiated with intravitreal aflibercept injections in the left eye.
Following two intravitreal aflibercept injections, OCT demonstrated complete resolution of the subretinal fluid and near-complete resolution of the intraretinal fluid, with only minimal residual intraretinal fluid remaining. Visual acuity improved from counting fingers at 1 meter at presentation to 20/100 (0.2 decimal visual acuity).
 Because no vitreous inflammation was present, systemic immunosuppressive therapy was not initiated. The patient remains under close follow-up. Additional immunomodulatory treatment may be considered in the future if inflammatory activity or recurrent disease develops.
Because no vitreous inflammation was present, systemic immunosuppressive therapy was not initiated. The patient remains under close follow-up. Additional immunomodulatory treatment may be considered in the future if inflammatory activity or recurrent disease develops.
Discussion
Punctate inner choroidopathy is an uncommon inflammatory chorioretinal disorder that predominantly affects young myopic women. It is characterized by multiple small yellow-white lesions located at the level of the inner choroid and retinal pigment epithelium, typically involving the posterior pole.
One of the most important complications of PIC is the development of choroidal neovascularization, which represents a major cause of visual loss. Anti-VEGF therapy has become the mainstay of treatment for PIC-associated choroidal neovascularization and often results in favorable anatomical and functional outcomes.
Differentiating PIC from multifocal choroiditis (MFC) can sometimes be challenging because both conditions belong to the spectrum of inflammatory chorioretinal disorders. However, the absence of vitritis is considered a hallmark feature of PIC, whereas vitreous inflammation is commonly observed in MFC. The lack of vitreous cells, absence of peripheral inflammatory lesions, and the characteristic multimodal imaging findings in our patient strongly supported the diagnosis of PIC rather than MFC.
Credit: M. Giray Ersoz, MD, FEBO, Retina Specialist
Memorial Bahçelievler Hospital, Department of Ophthalmology, Istanbul, Turkey
Arel University School of Medicine, Department of Ophthalmology, Istanbul, Turkey
Instagram accounts: @retina.review and @retina.dr.girayersoz
Website: www.girayersoz.com.tr
