
A 43-year-old female patient presented with gradually progressive visual decline in both eyes. She denied photophobia or other visual disturbances. Her past medical history was notable for Hashimoto thyroiditis, and there was no significant family history of ocular disease.
On ophthalmic examination, best-corrected visual acuity (BCVA) was 8/10 in both the right and left eyes. Color vision testing using Ishihara plates was normal (24/24 in both eyes). Intraocular pressure was 18 mmHg bilaterally. Anterior segment examination was unremarkable in both eyes.
The patient did not report headache, and neurological evaluation performed at an external center was unremarkable. Brain magnetic resonance imaging (MRI), magnetic resonance angiography (MRA), and magnetic resonance venography (MRV) were all reported as normal.
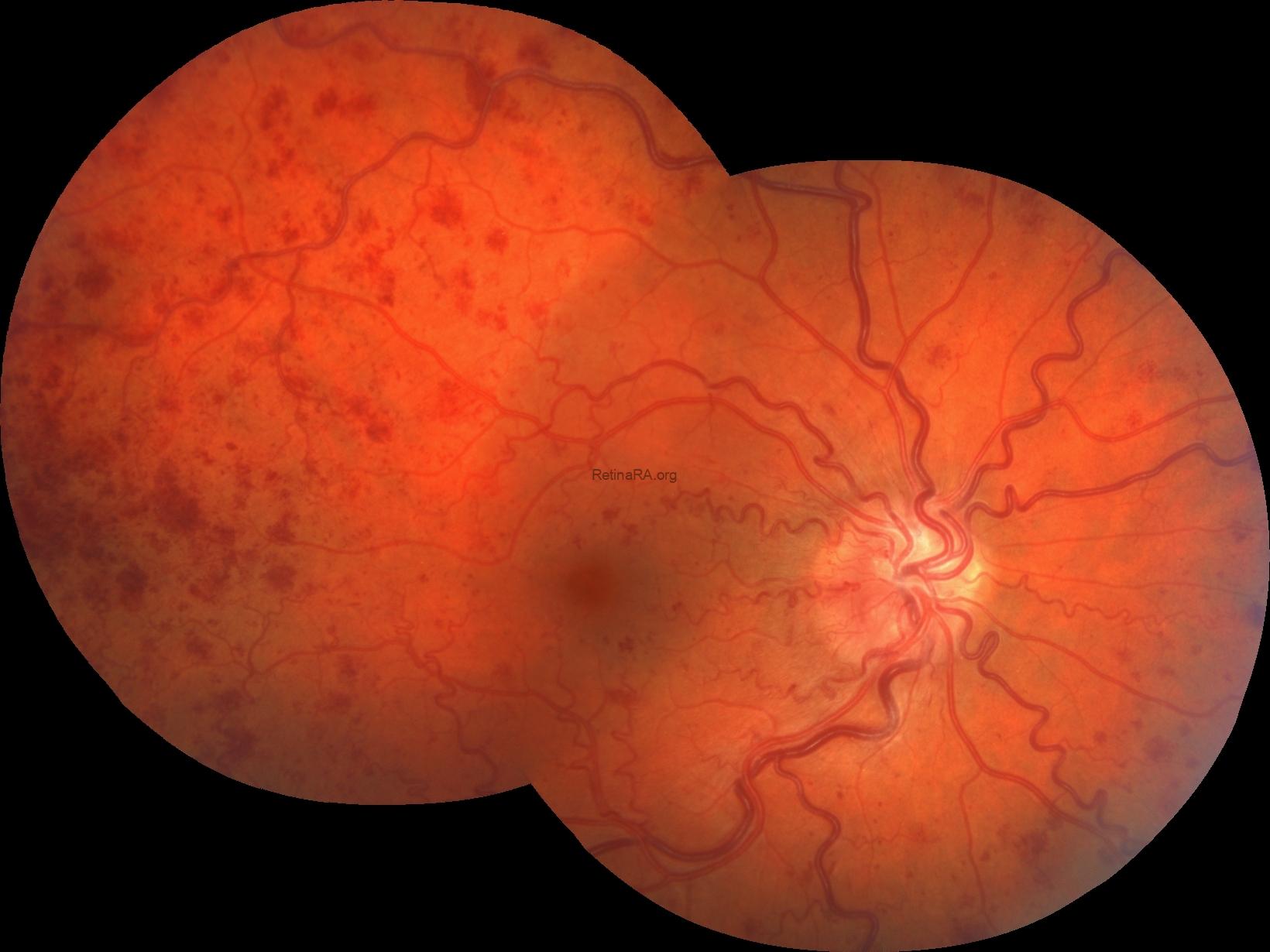

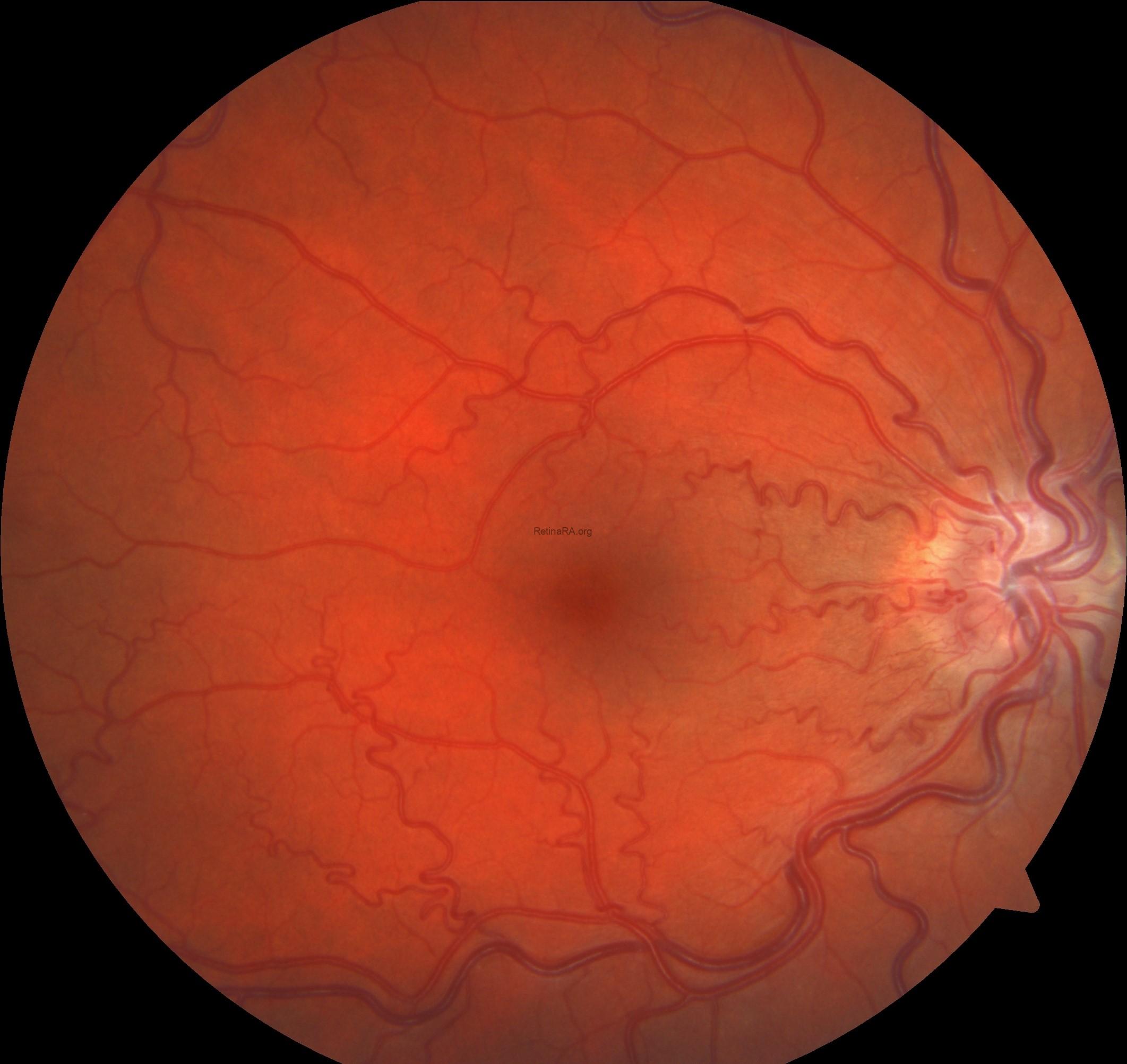
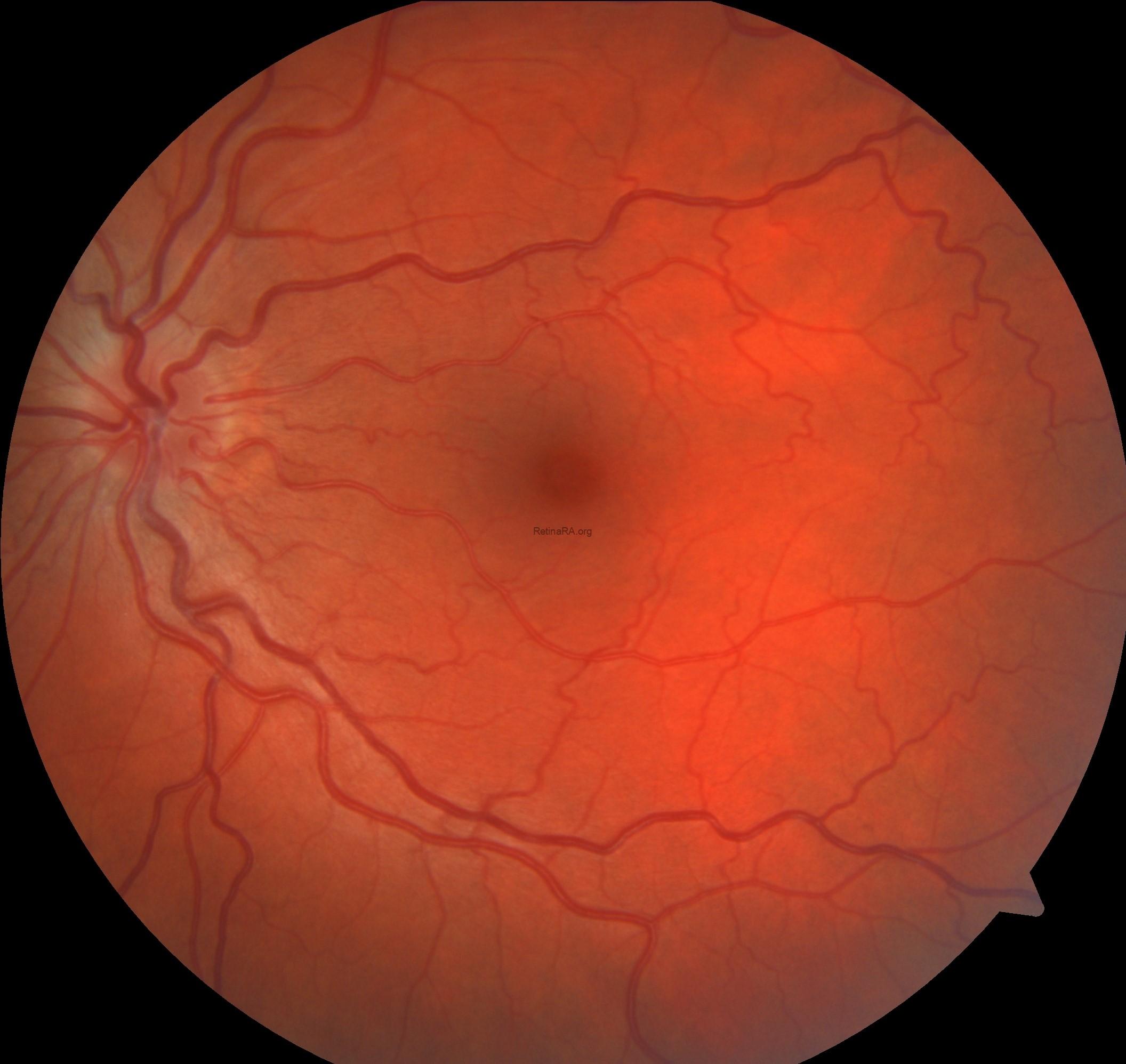
Color fundus photography revealed indistinct margins of the right optic disc with an edematous appearance. Increased vascular tortuosity, particularly marked arterial tortuosity, was observed. The retina was diffusely covered with hemorrhages.
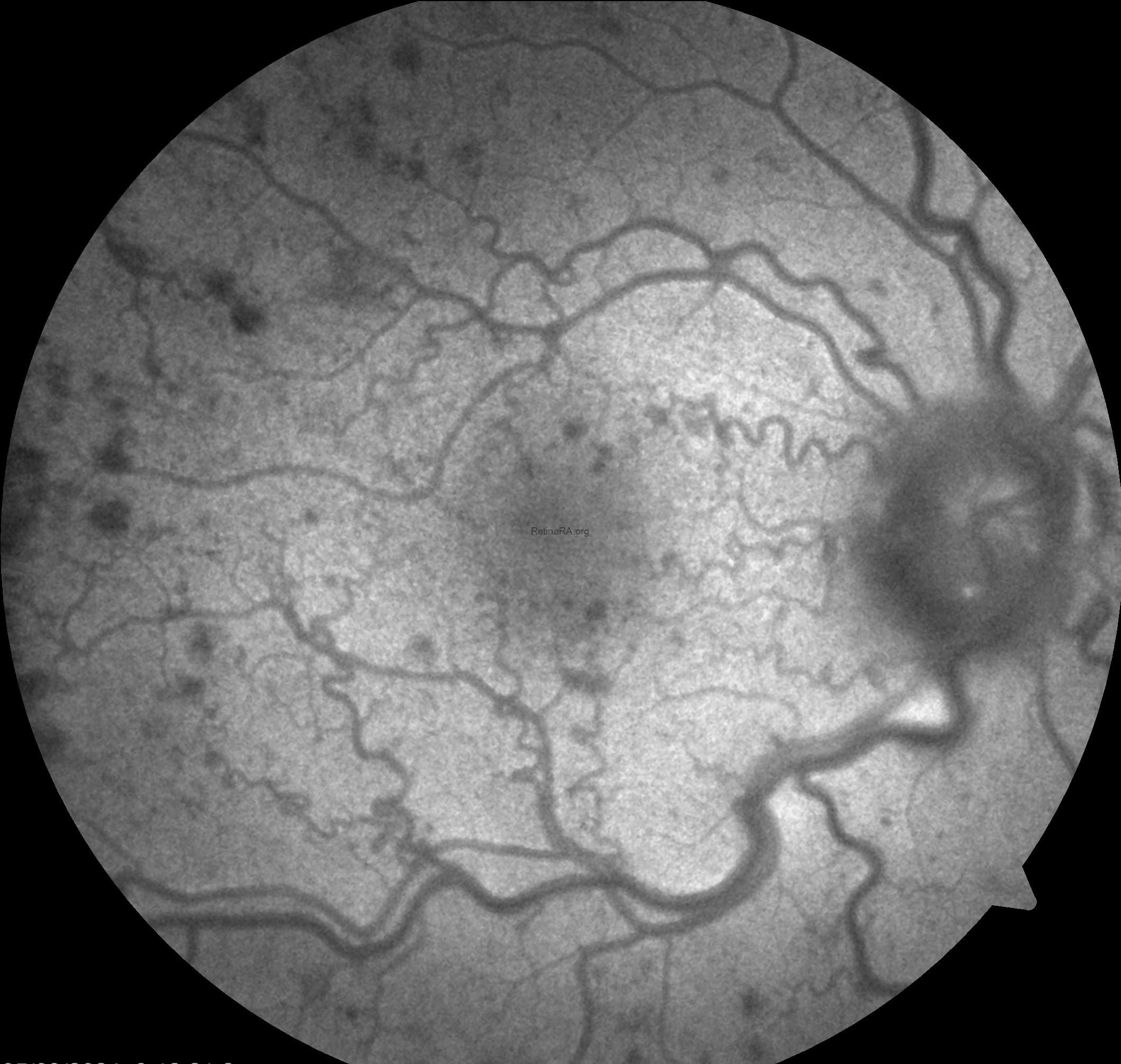

Fundus autofluorescence (FAF) imaging showed no abnormalities other than the hemorrhages.
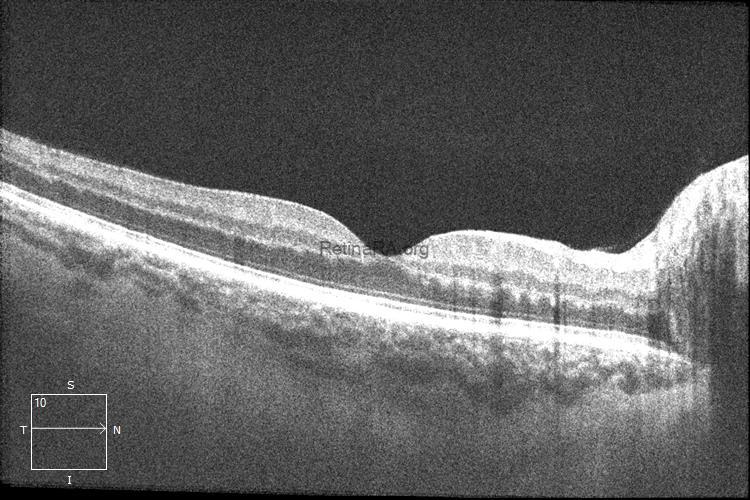
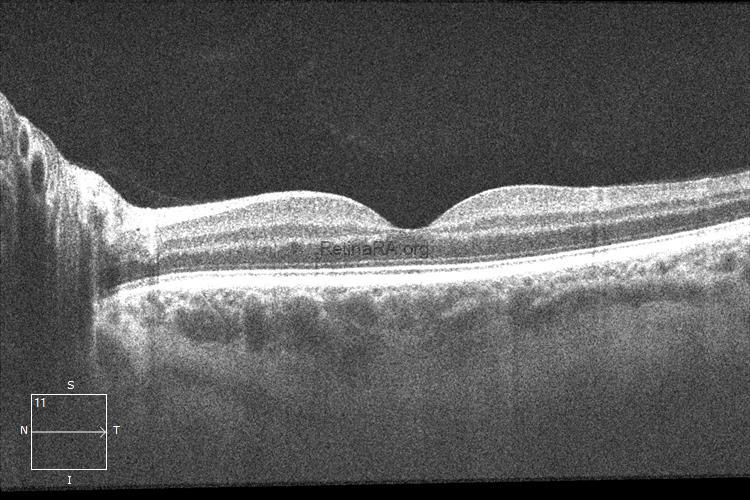
In the right eye, more prominent irregularities related to hemorrhage were observed in the outer plexiform and Henle fiber layers.
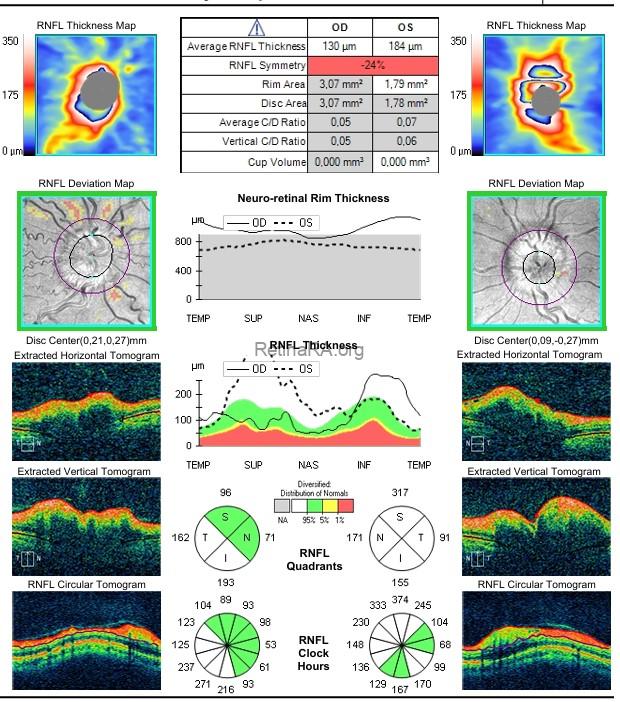
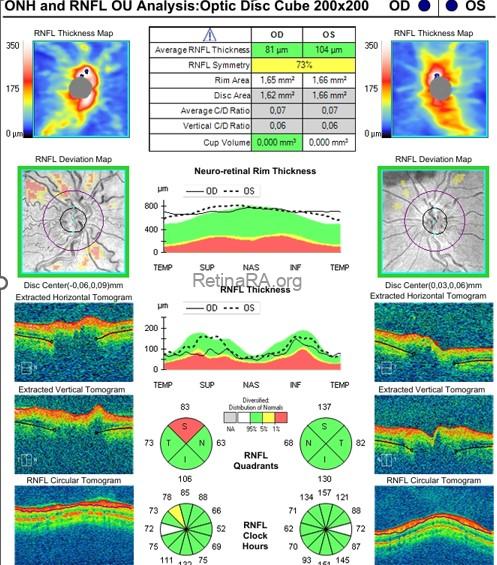
OCT optic disc and RNFL analysis demonstrated bilaterally elevated optic disc margins, with increased retinal nerve fiber layer (RNFL) thickness in all quadrants.
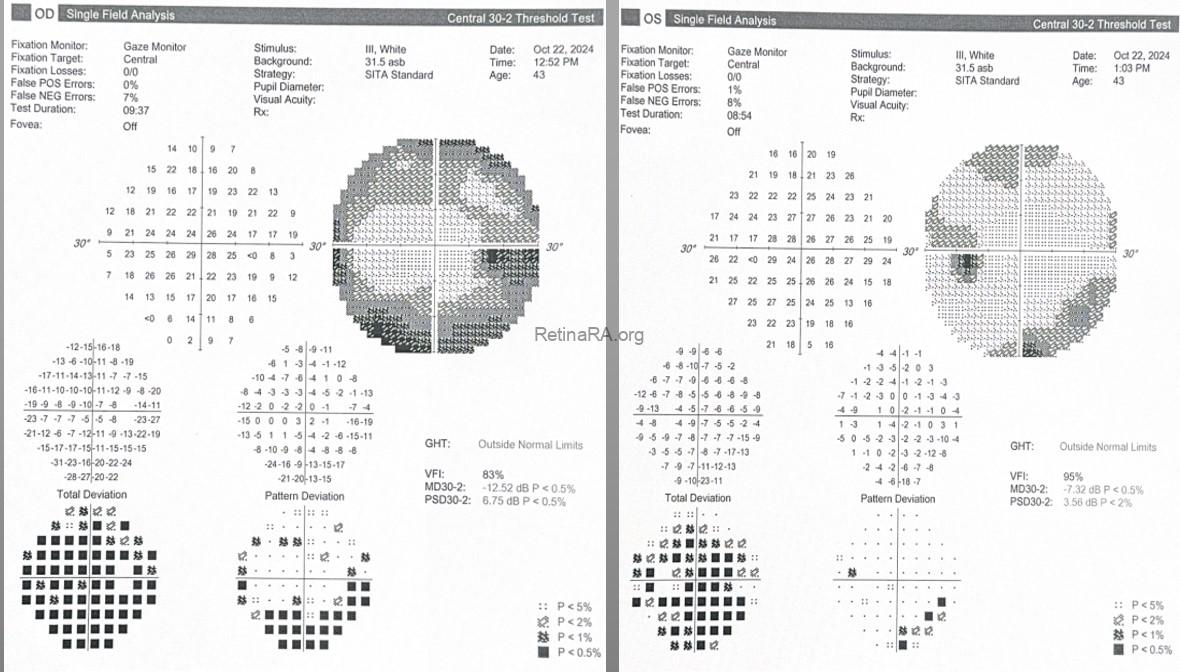
On visual field testing, the right eye (OD) demonstrated a widespread peripheral visual field defect. Corresponding significant depressions were observed in these areas on the pattern deviation map. Bilateral enlargement of the blind spot was also noted.
Based on the preliminary diagnosis of Papilledema secondary to headache-free chronic idiopathic intracranial hypertension and partial retinal venous stasis (right eye), a neurology consultation was requested. Lumbar puncture was performed, and the opening cerebrospinal fluid (CSF) pressure was measured at 280 mmH₂O. The patient was started on oral acetazolamide therapy. At the 3-month follow-up, a marked improvement in clinical findings was observed.
At the final follow-up examination, there was a marked regression of optic disc edema.
Idiopathic intracranial hypertension (IIH) is a disorder characterized by elevated intracranial pressure without an identifiable structural or vascular cause. Although headache is the most common presenting symptom, a subset of patients may present without headache, making diagnosis more challenging and often delayed. In such cases, visual symptoms or incidental detection of papilledema may be the initial clinical finding. Headache-free IIH has been reported in the literature as a less typical presentation, yet it carries a similar risk of visual morbidity due to sustained optic nerve head edema. Therefore, recognition of this atypical presentation is critical, particularly in patients with unexplained bilateral optic disc swelling and normal neuroimaging, to ensure timely diagnosis and appropriate management.
Credit: M. Giray Ersoz, MD, FEBO
Memorial Hospital, Department of Ophthalmology, Istanbul, Turkey
Arel University School of Medicine, Department of Ophthalmology, Istanbul, Turkey
Instagram accounts: @retina.review and @retina.dr.girayersoz
and Sepideh Lotfi, MD
Biruni University School of Medicine, Department of Ophthalmology, Istanbul, Turkey
Instagram accounts: @sepidls
