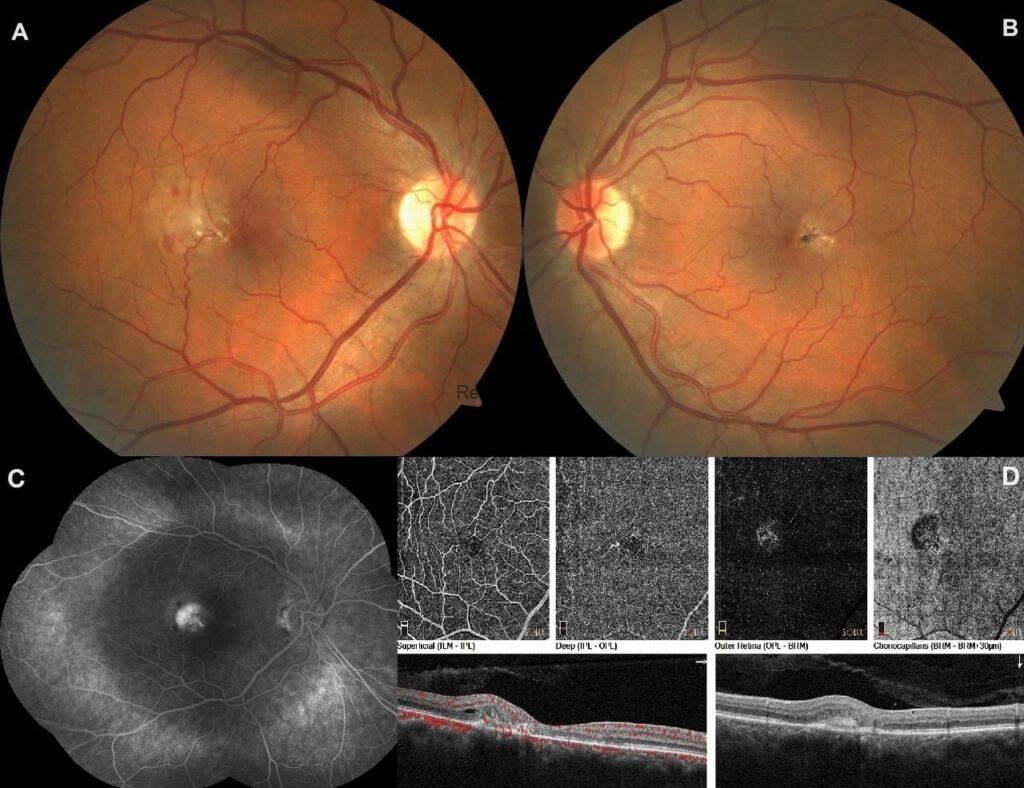
A 50-year-old male applied with decreased vision in his right eye. The best corrected visual acuities were 20/70 in the right eye and 20/25 in the left eye. Fundus examinations demonstrated parafoveal loss of transparency, right angle venules and telangiectatic vessels that are more prominent temporally in the macula of both eyes in addition to a dirty grayish retinal neovascular membrane with retinal hemorrhages temporal to the fovea of the right eye, besides retinal pigment epithelium (RPE) atrophic changes, RPE hyperplasia, and yellowish crystalline deposits in the macula of the left eye.


Fundus fluorescein angiography of the right eye showed staining of temporal parafoveal capillaries and the presence of a juxtafoveal choroidal neovascularization.

Optical coherence tomography angiography of the right eye exhibited the telangiectatic vessels in the superficial and deep retinal plexus, neovascular membrane with composed of loops, peripheral anastomoses and surrounded by a hypointense halo in the outer retina and choriocapillaris slabs in addition to subretinal hyperreflective material with intraretinal fluid in the B-scan.

Idiopathic macular telangiectasia Type 2 is bilateral and characterised by retinal opacification, vascular telangiectasia, right-angled venules, intraretinal crystalline deposits, foveal thinning, retinal pigment epithelial hypertrophy and rarely, choroidal neovascularisation (proliferative form). Active macular neovascularization is clinically suspected in the presence of subretinal hemorrhage, thickening of the retina and/or visible membrane at the macula. Macular neovascularizaiton can easily be confirmed confirmed with fundus fluorescein angiography and optical coherence tomography angiography imaging.
Credit: Kemal Tekin, M.D., from Ulucanlar Eye Training and Research Hospital
Instagram accounts: @retina.academy and @dr.kemaltekin
