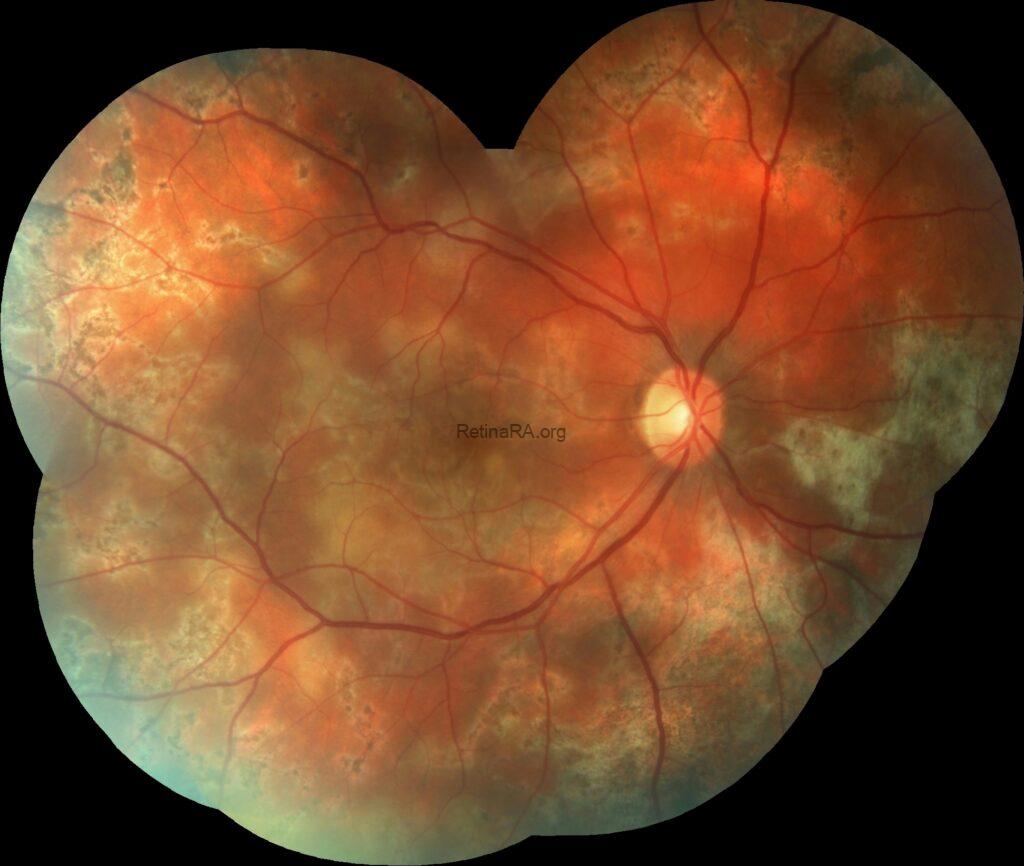
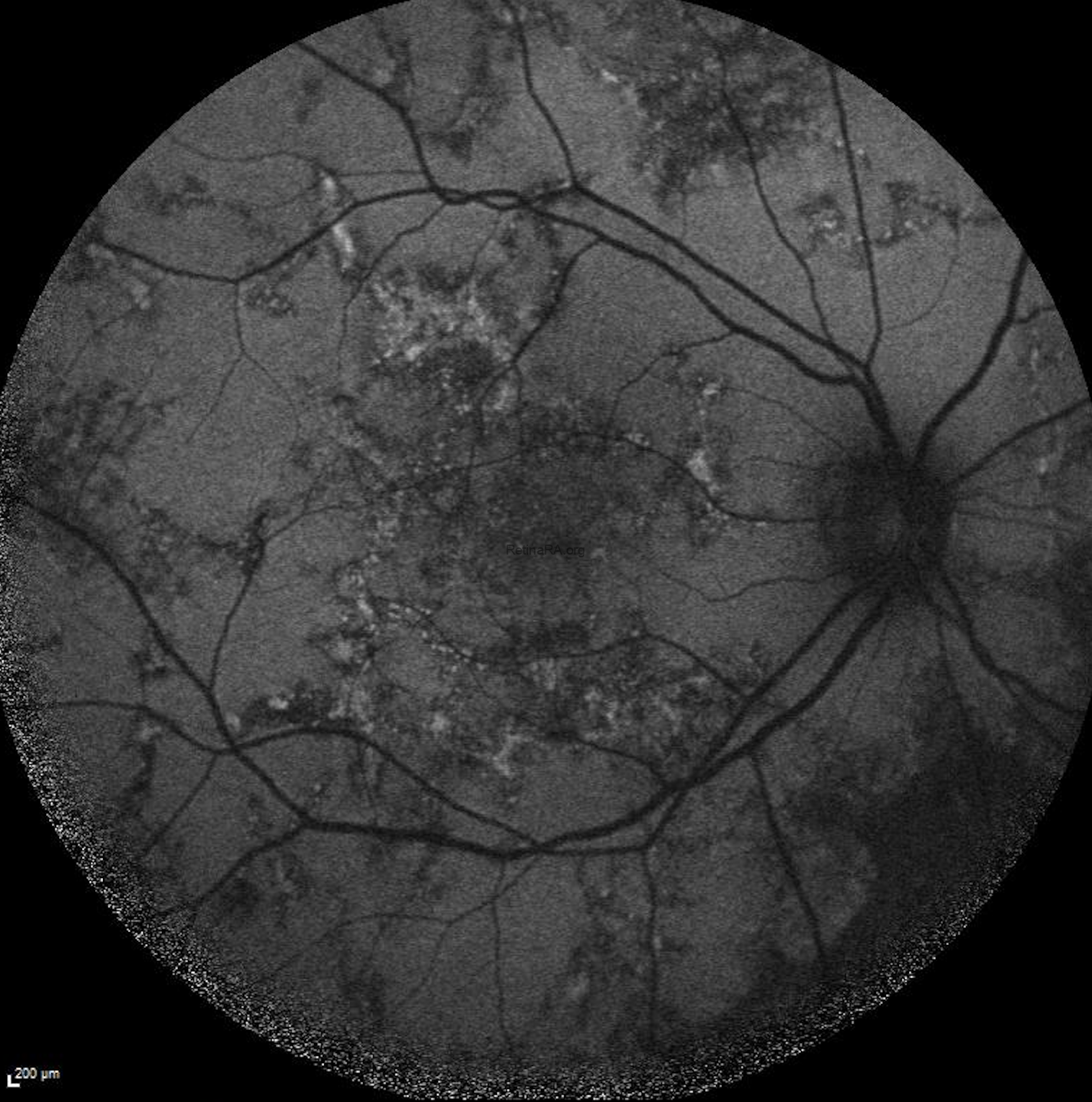
A 45-year-old male patient presented with blurred vision in the right eye. Visual acuity was 0.8/1.0 in right and left eyes, respectively. At the time of presentation, the left eye color fundus photographs show multiple, grayish yellow lesions with unclear borders.


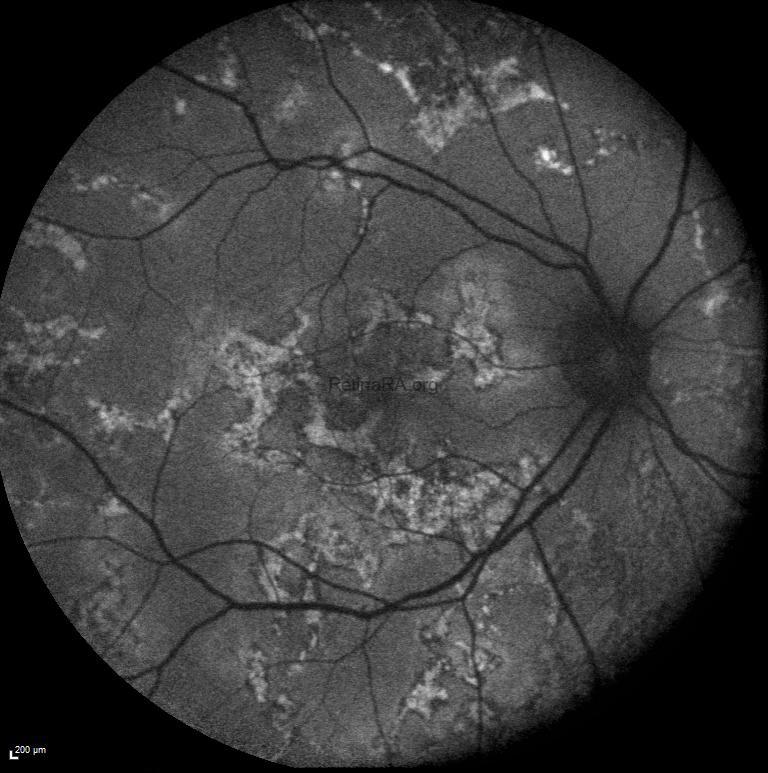
It is noteworthy that active lesion margins are hyperautofluorescent on FAF imaging.

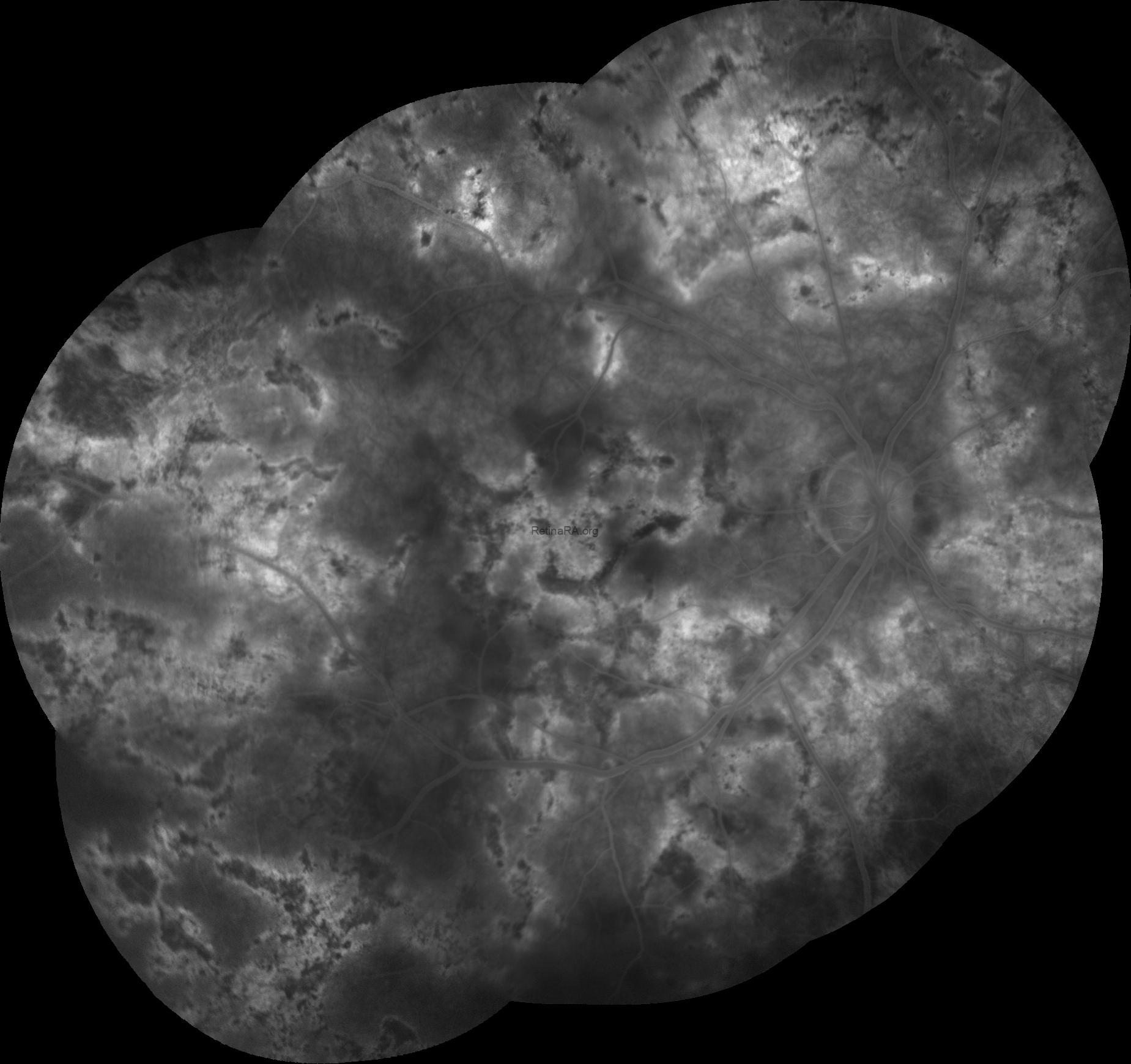
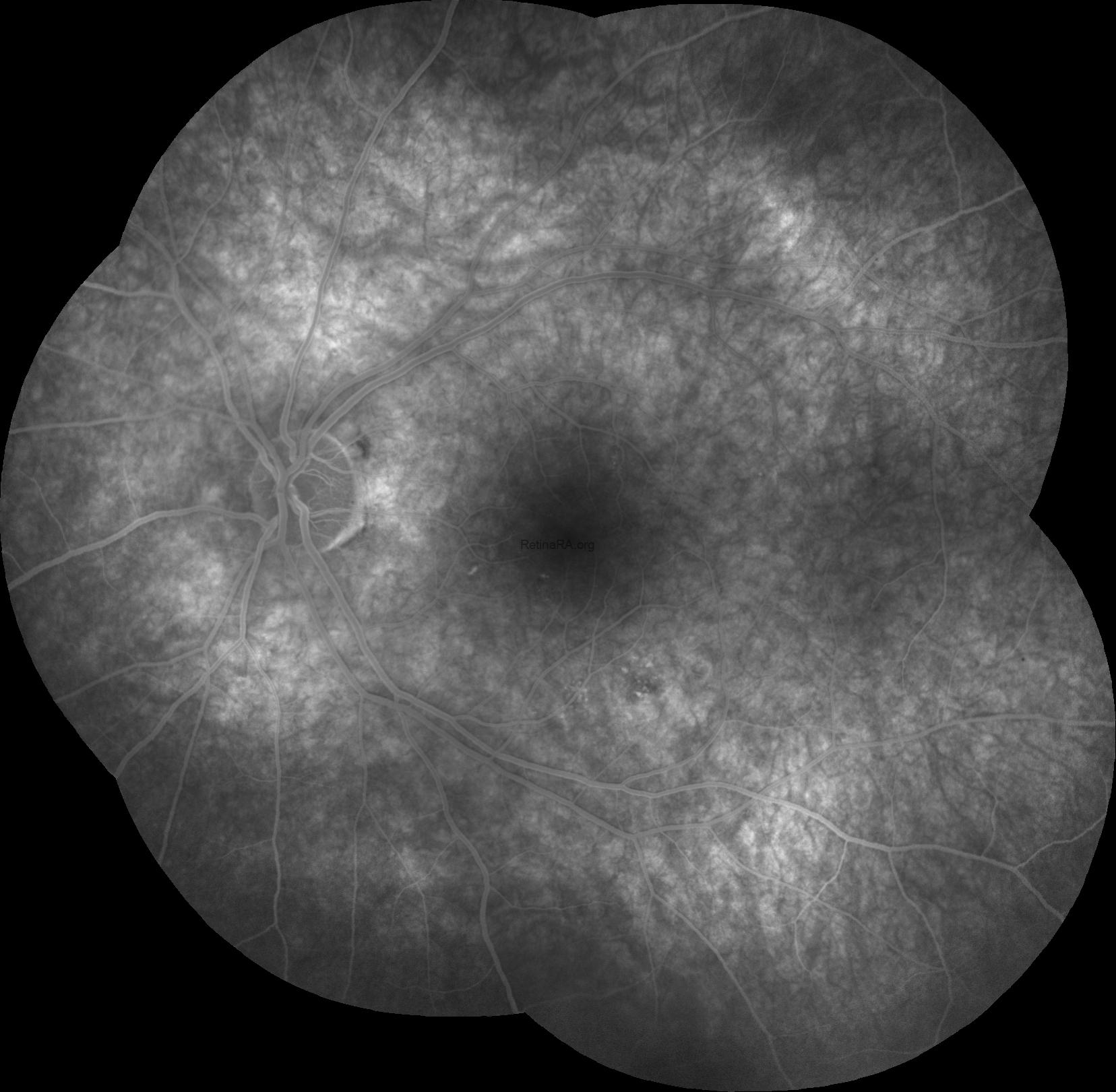
FFA shows a marked hyperfluorescence at the lesion margins.
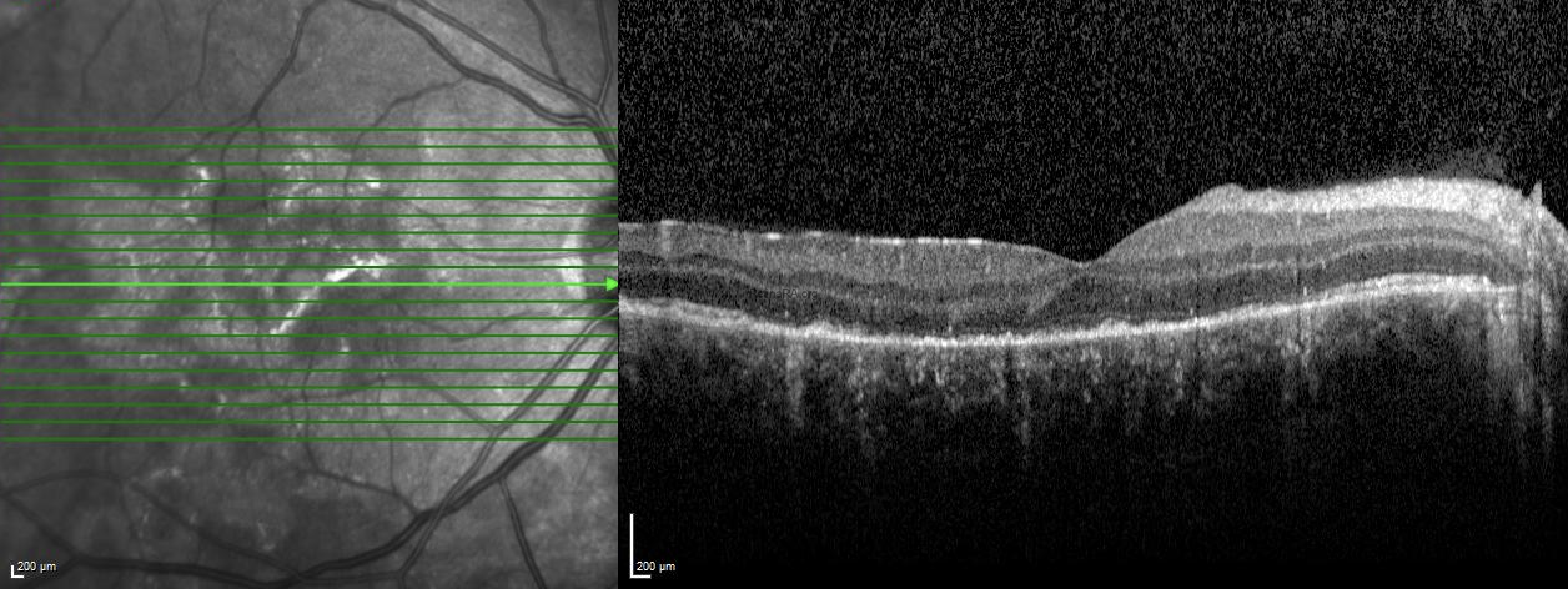
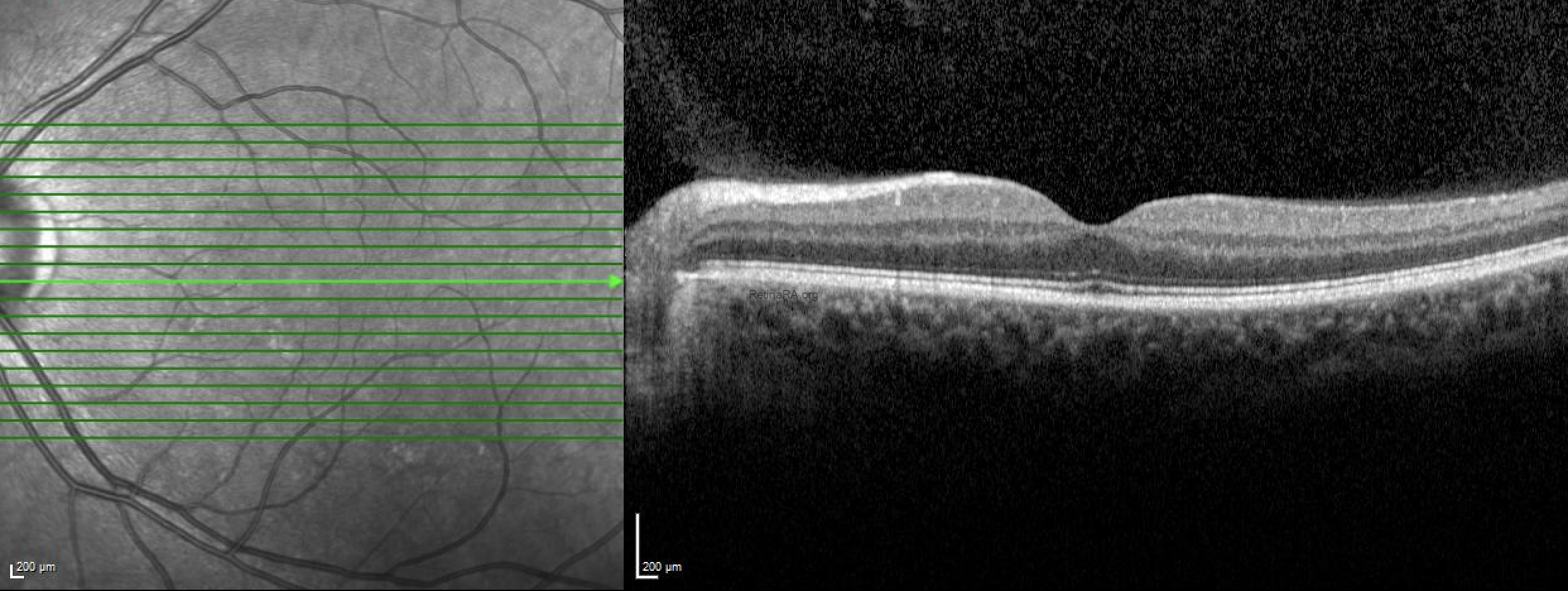
OCT sections show outer retinal atrophy and associated hyperreflectivity in the choroid.
The quantiferon-TB test was positive and the patient was diagnosed with Tubercular serpiginous‑like choroiditis. Anti tubercular treatment (ATT) was started and then oral steroid was added. Healed lesions showed hypoautofluorescence on FAF.
Tubercular serpiginous‑like choroiditis (TB SLC) is characterized by multifocal, initially discrete and later confluent, yellowish lesions, mostly noncontiguous to the optic disc, with slightly raised edges, showing active edge wave‑like progression and central healing. TB SLC can be unilateral or bilateral, and it is commonly associated with mild vitritis. In TB SLC even one positive immunologic evidence, namely a positive PPD skin test or interferon gamma release assay (IGRA), not supported by radiologic findings, is considered enough to start ATT. Systemic corticosteroids could be initiated concomitantly with or soon after the administration of ATT in patients with TB SLC.
Credit: Merve İnanç Tekin, MD, FEBO
Ulucanlar Eye Training and Research Hospital, Ankara, Turkey
Instagram accounts: @uveacademy and @merveinanctekin