A 77-year-old man was referred to the retina clinic due to blurred and decreased vision in his right eye. It was learnt that the patient underwent a standard uncomplicated cataract surgery two-months ago. The BCVAs were 20/50 in the right eye and 20/30 in the left eye. IOP s were within normal limits. Anterior segment examinations revealed the completely normal posterior chamber IOL in the right eye and nuclear sclerosis in the left eye.
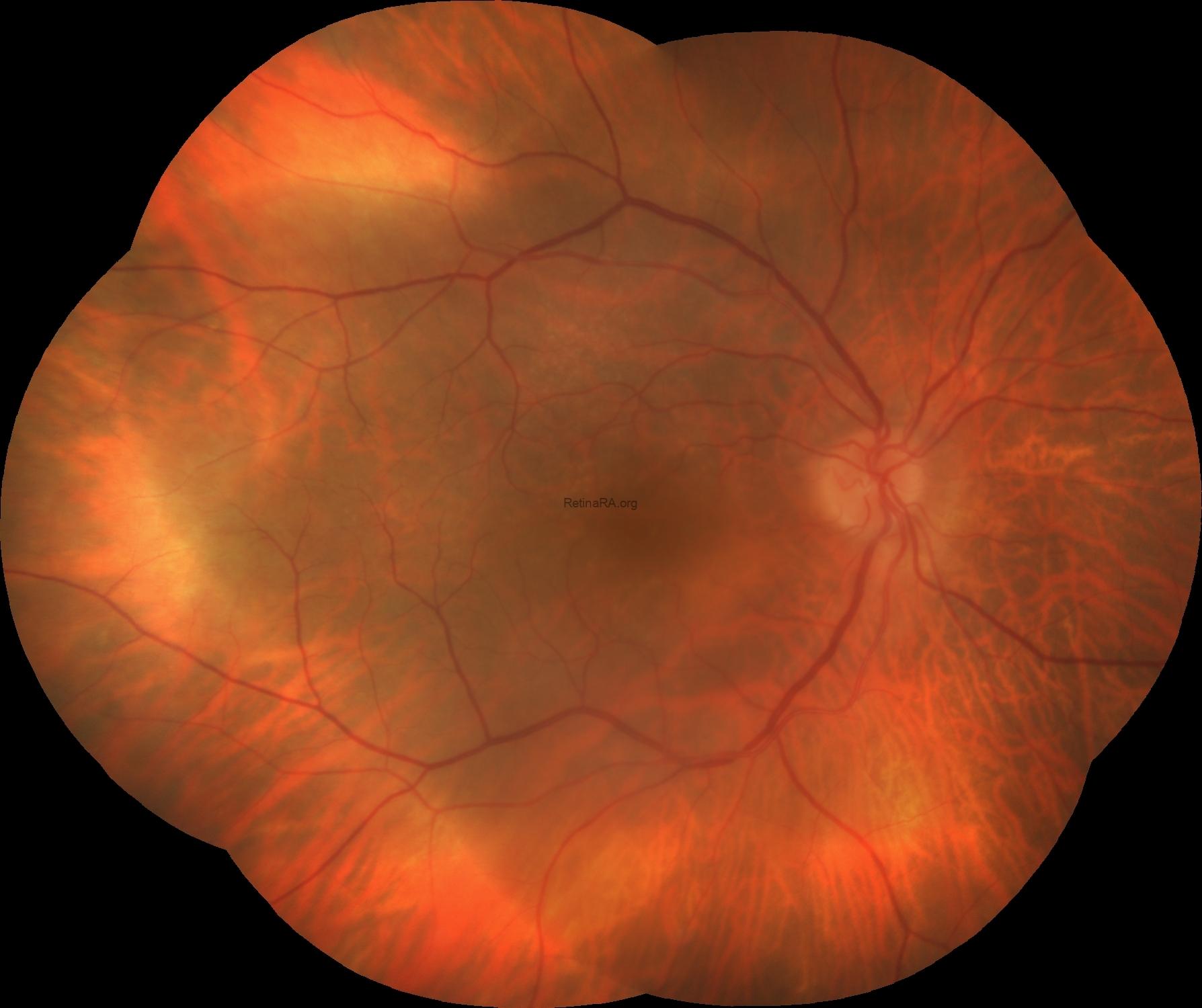
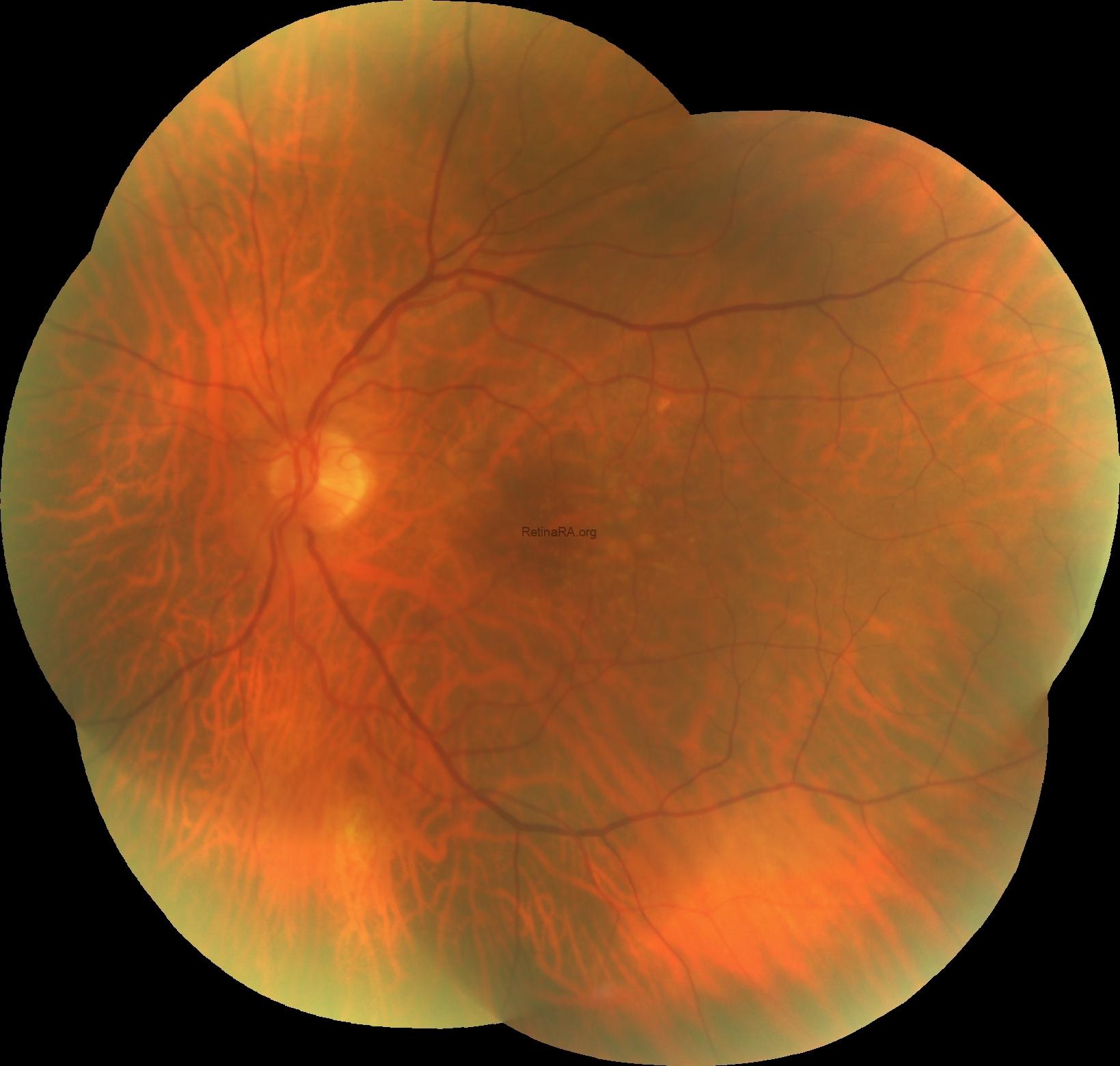
Dilated fundus examination demonstrated small and medium sized drusen in both eyes.
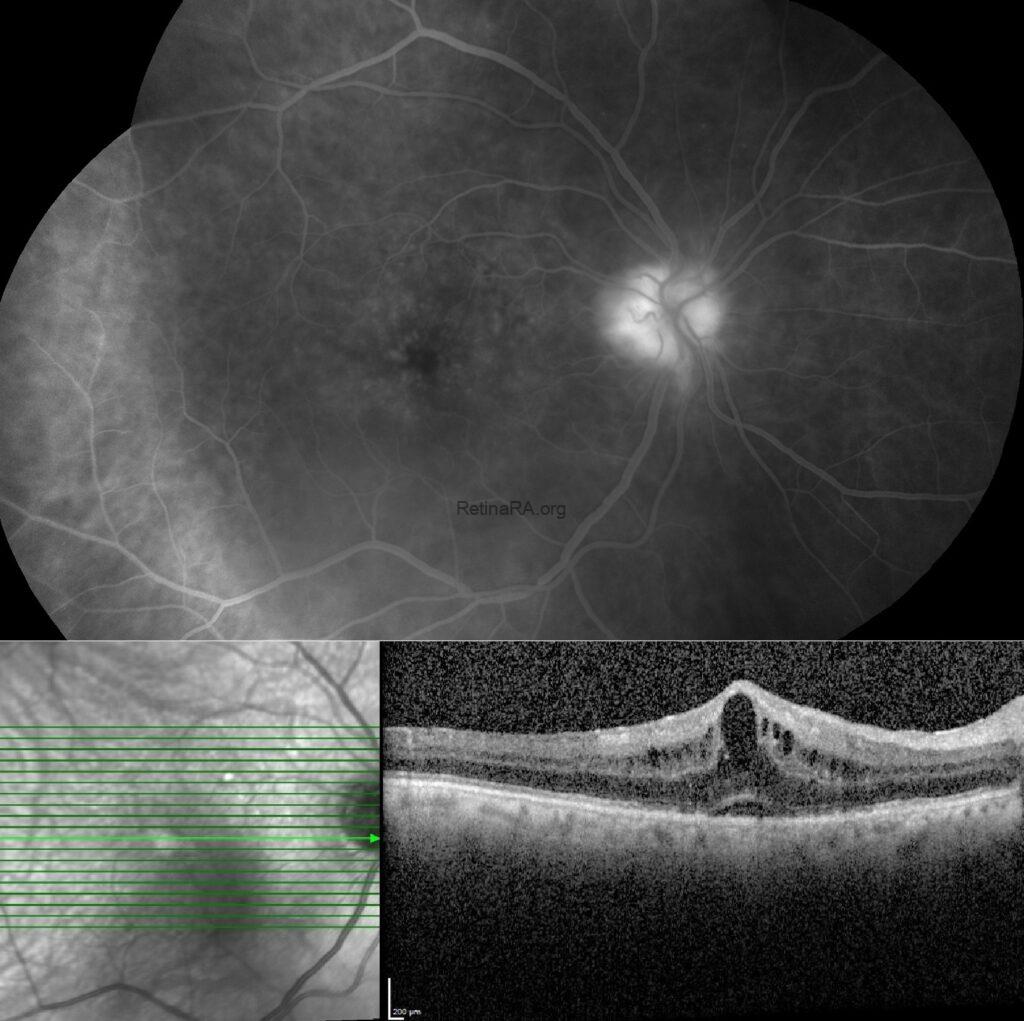
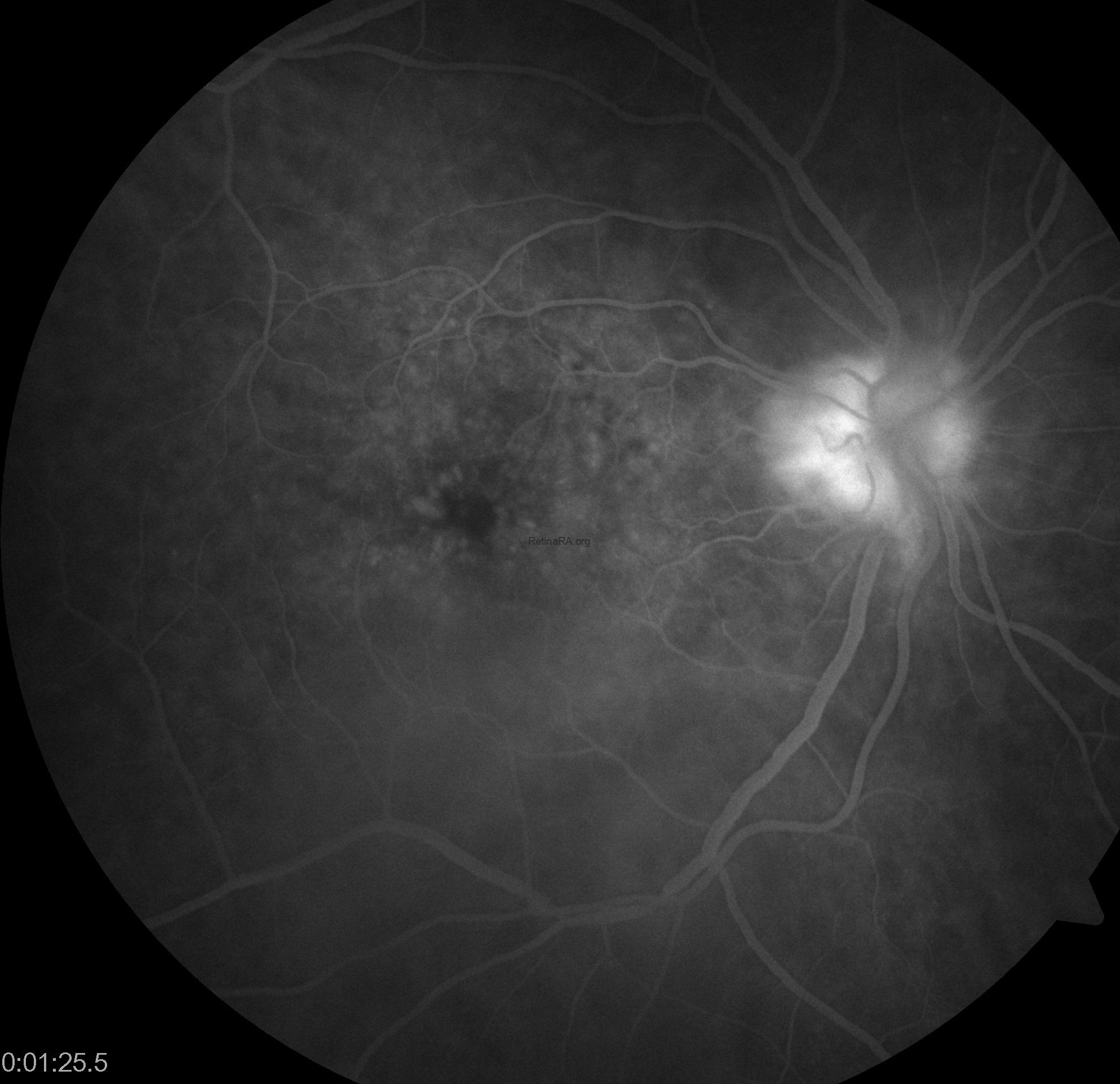
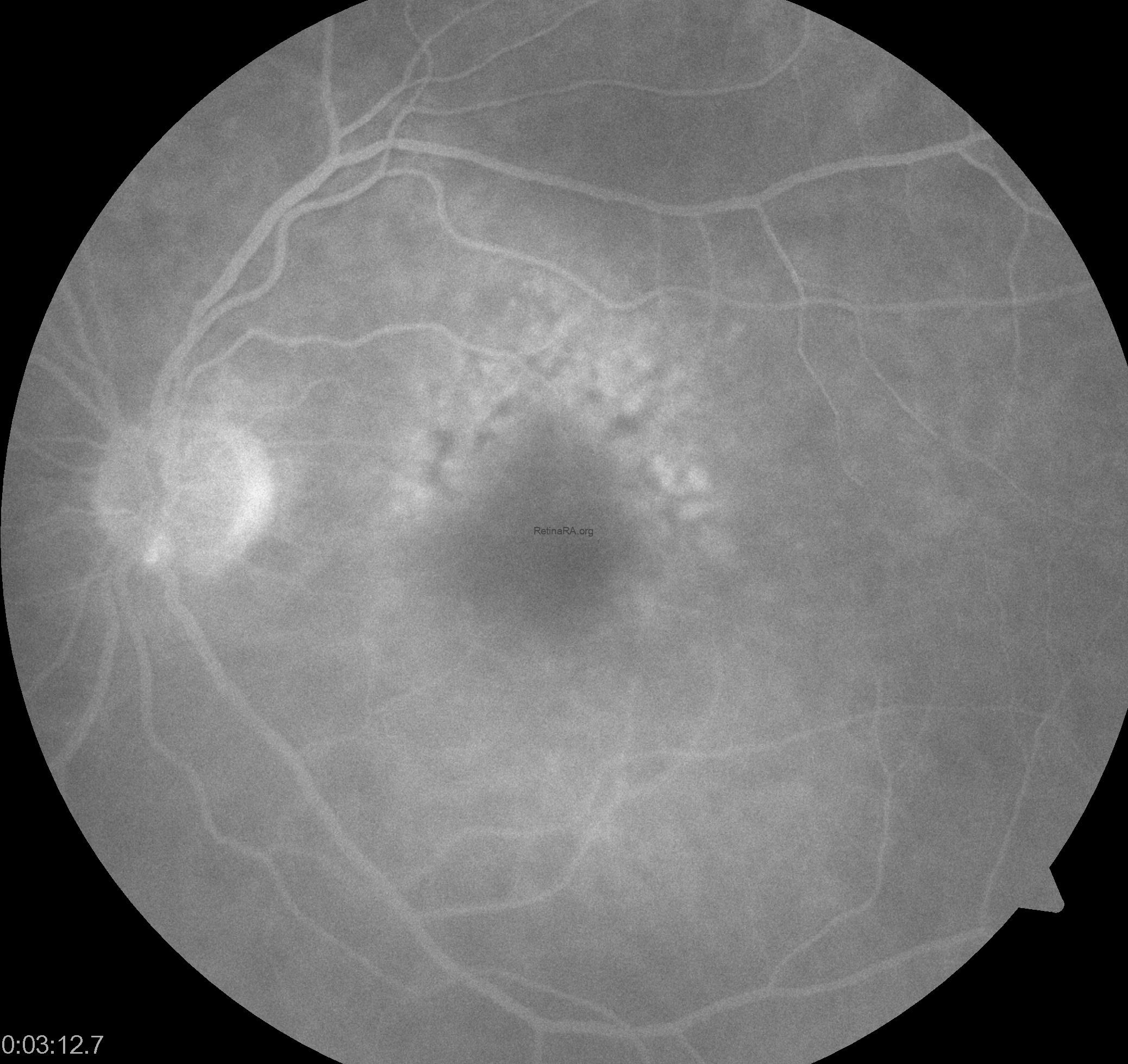
Fundus fluorescein angiography revealed petaloid pattern of hyperfluorescence at the fovea in the late phases in addition to optic nerve staining in the right eye, and patchy hyperfluorescence due to staining of drusen in both eyes.

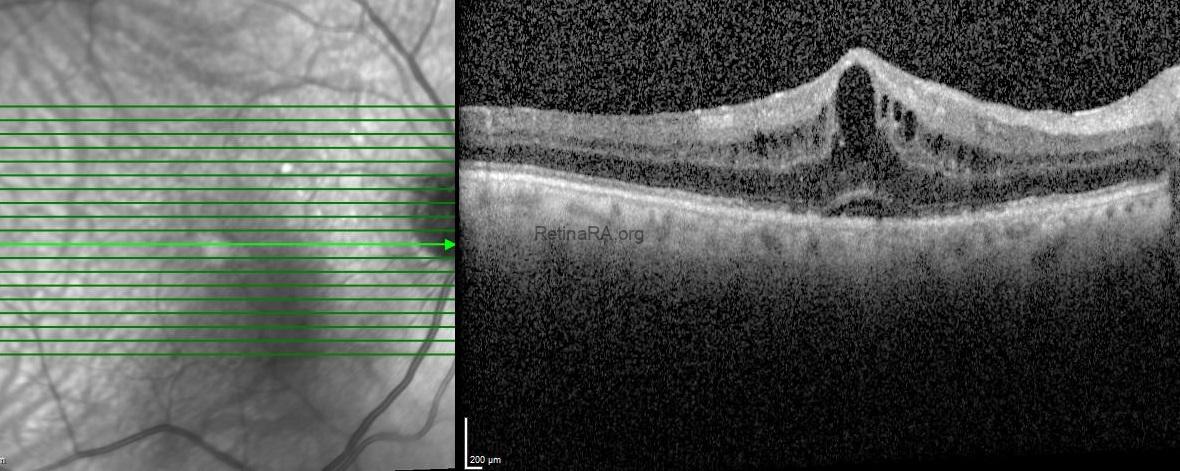
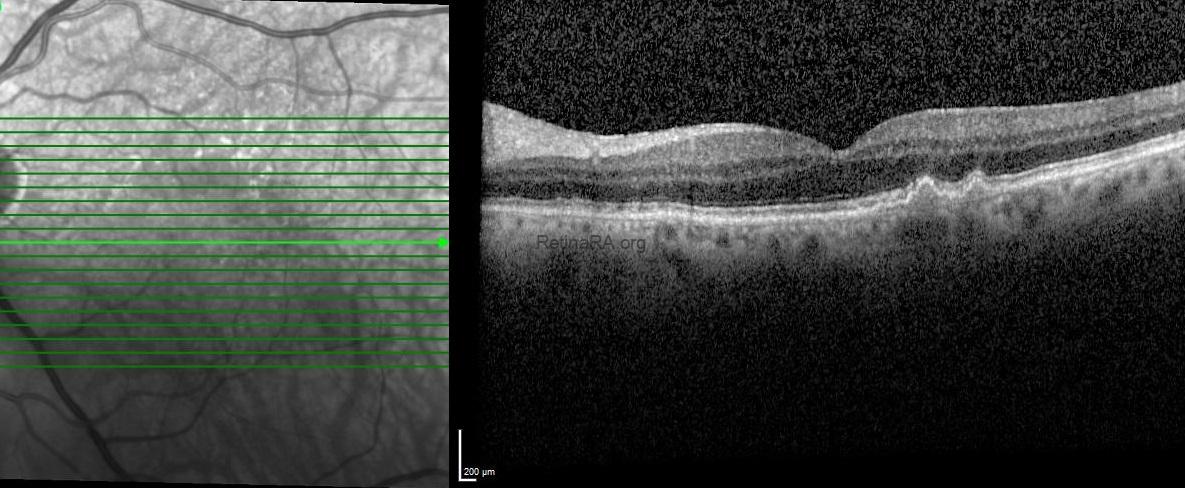
Optical coherence tomography (OCT) exhibited retinal thickening, intraretinal cystic spaces and serous retinal detachment in the right eye and subretinal drusenoid deposits and drusenoid pigment epithelium detachment with normal foveal contour in the left eye.
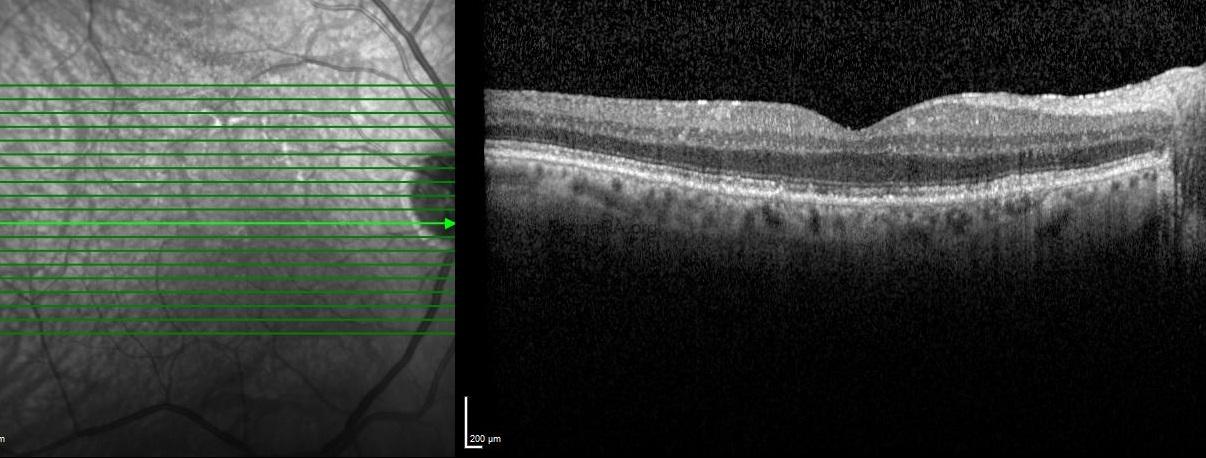
The patient was diagnosed as pseudophakic cystoid macular edema also known as Irvine-Gass syndrome and topical nepafenac 0.1% eye drops
3 times per day was recommended. One-month after the topical treatment, the BCVA of the right eye improved to 20/25 and OCT showed the complete resolution of subretinal and intraretinal fluid.
Pseudophakic cystoid macular edema, also known as Irvine-Gass syndrome, is one of the most common causes of painless decreased vision following even uneventful cataract surgery. The pathogenesis is multifactorial and its incidence is higher in patients with vasculopathy, hypertension, and uveitis. It is thought that inflammatory mediators (mainly prostaglandins) are upregulated in the aqueous and vitreous humors after surgical manipulation and inflammation breaks down the blood-aqueous and blood-retinal-barriers, which leads to increased vascular permeability. Clinical practice and theoretical background support topical non-steroidal anti-inflammatory drugs as the first-line therapy. Invasive procedures, such as periocular steroids, intravitreal corticosteroids, and anti-vascular endothelial growth factor are usually applied in prolonged or refractory cases.
Credit: Kemal Tekin, M.D., from Ulucanlar Eye Training and Research Hospital
Instagram accounts: @retina.academy and @dr.kemaltekin