This was a 55-year-old woman with systemic lupus erythematosus treated with 400 mg/kg hydroxychloroquine daily for 6 years (daily dose, 5.72 mg/real body weight or 6.5 mg/kg ideal body weight; cumulative dose, 876 g) experienced progressive central visul defect and a scotoma affecting her reading ability. The BCVAs were 20/30 for both eyes and the IOPs were within normal limits. Anterior segment examinations were also normal except mild nuclear sclerosis for both eyes.
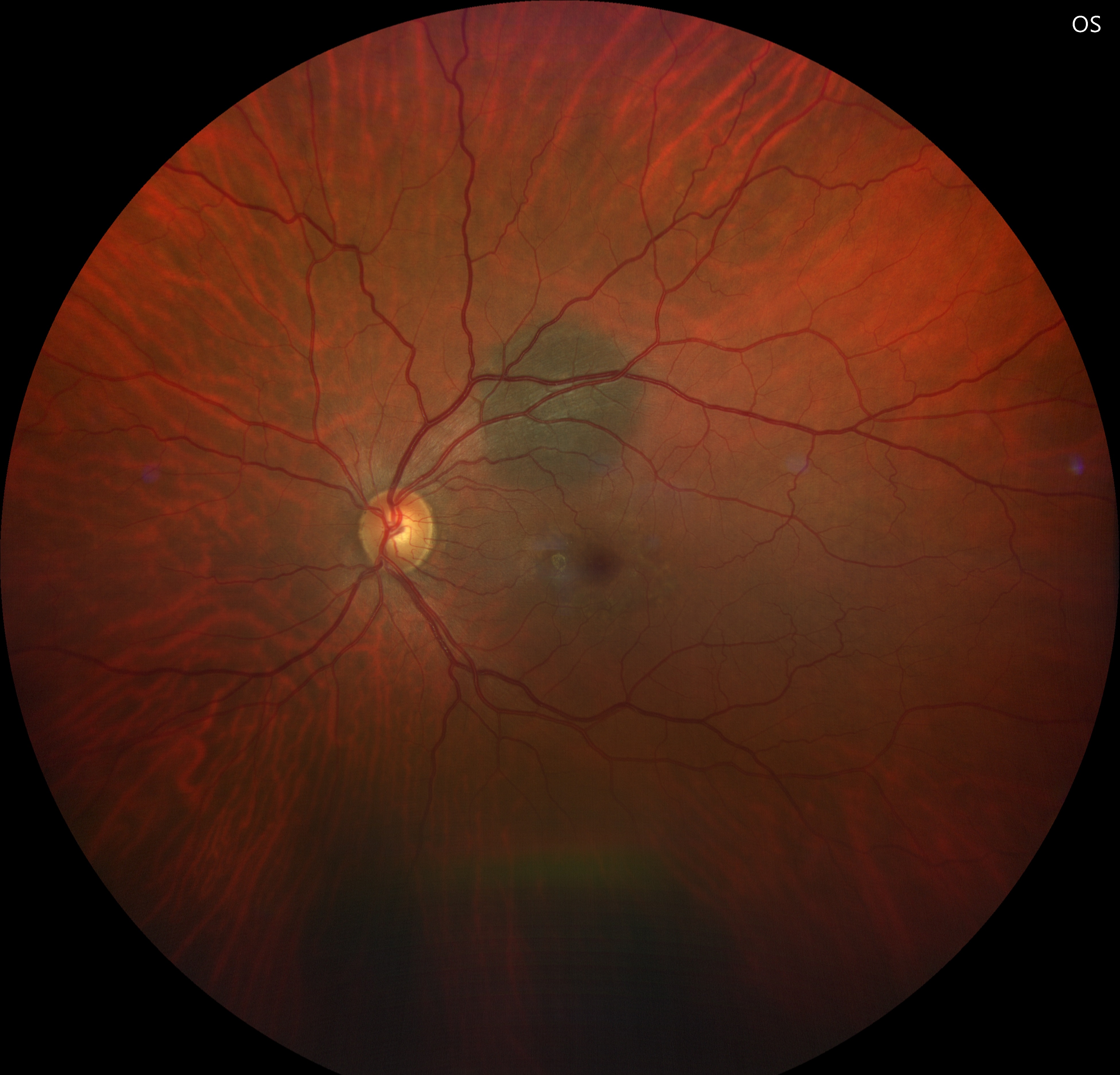
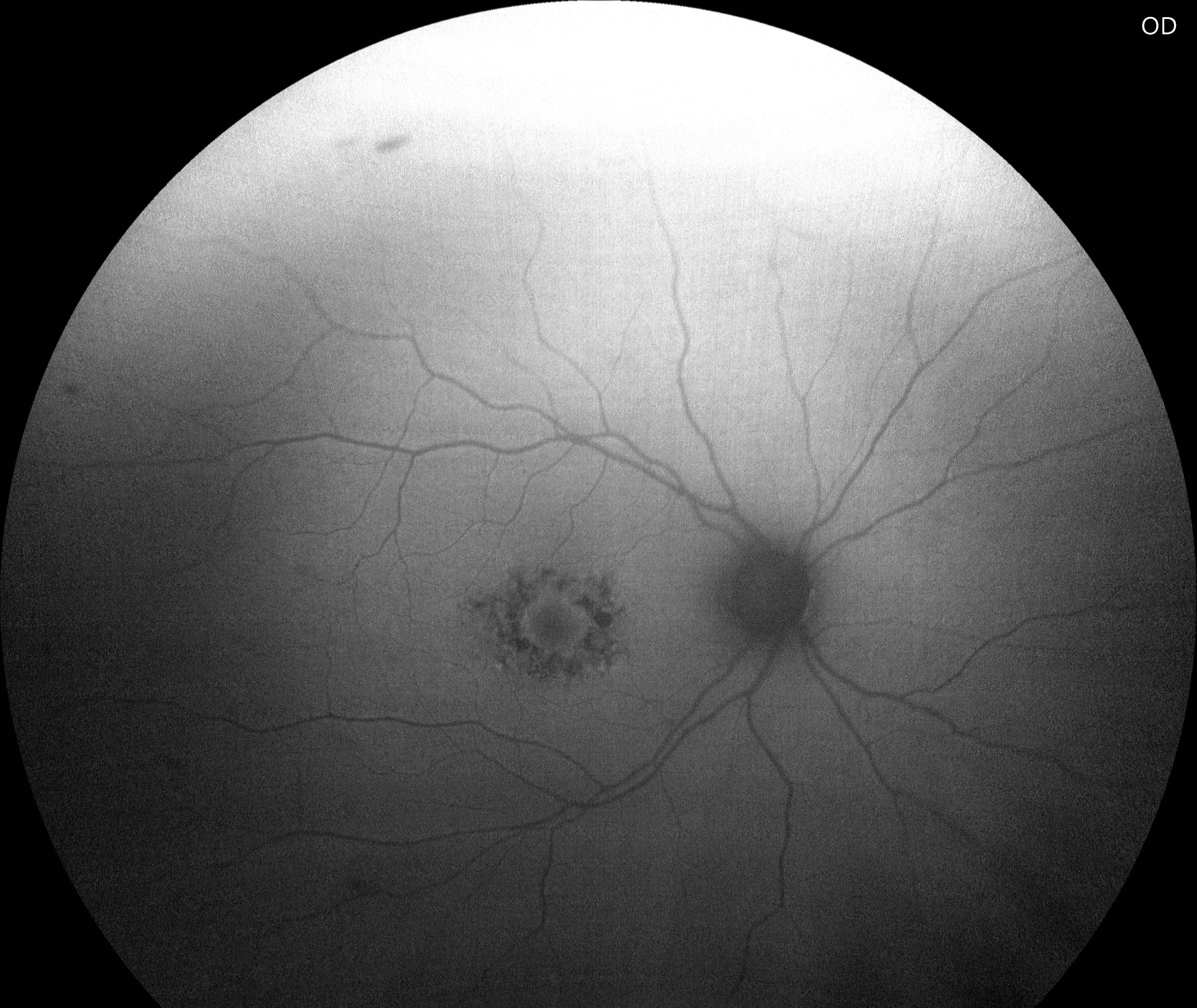
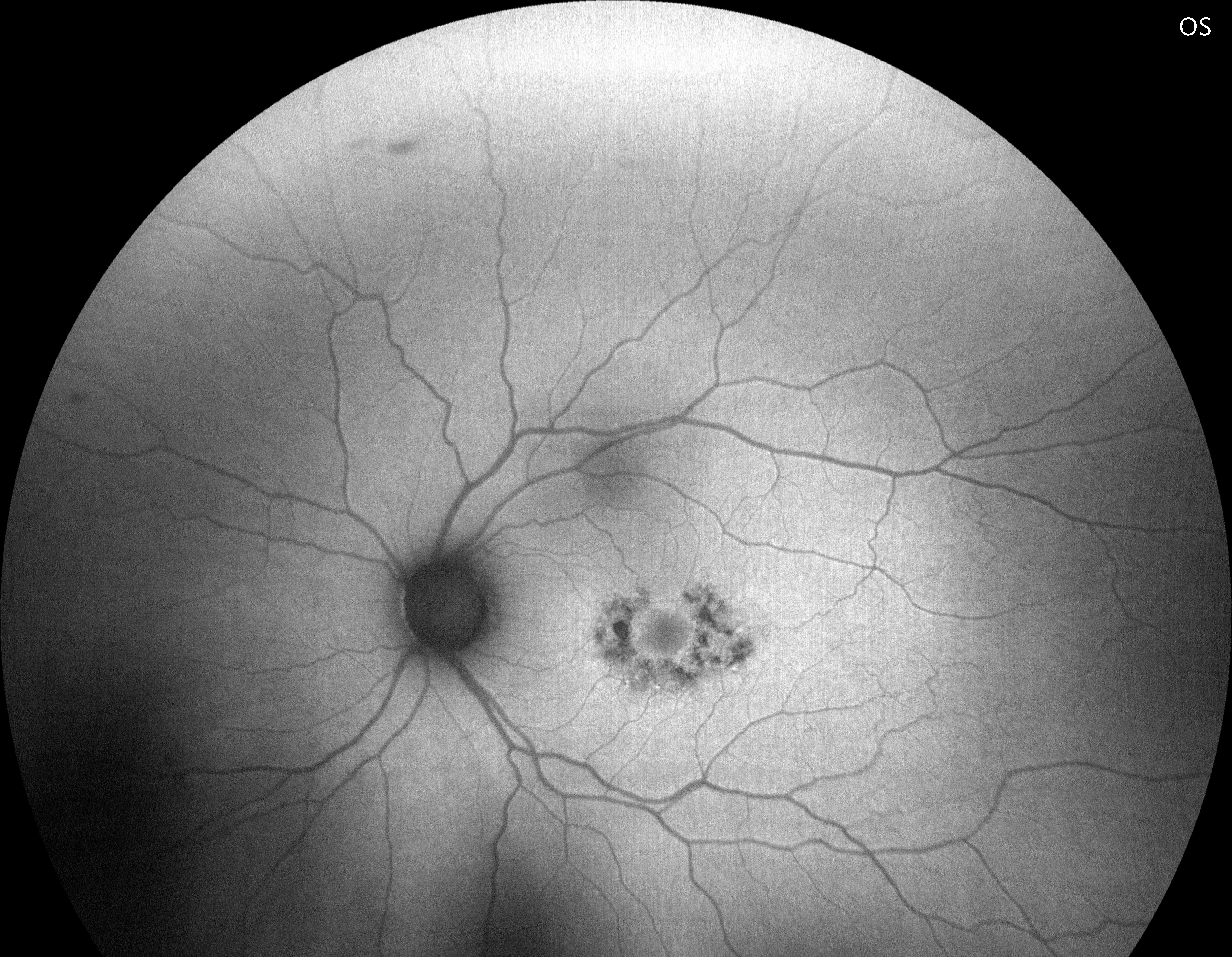
Dilated fundus examination showed bilateral pafoveal pigmentary alterations indicating the bull’s-eye maculopathy in both eyes in additon to a flat choroidal nevus approximately 3 disc-diameter in size along the superior arcade with overlying drusen and no observable lipofuscin.


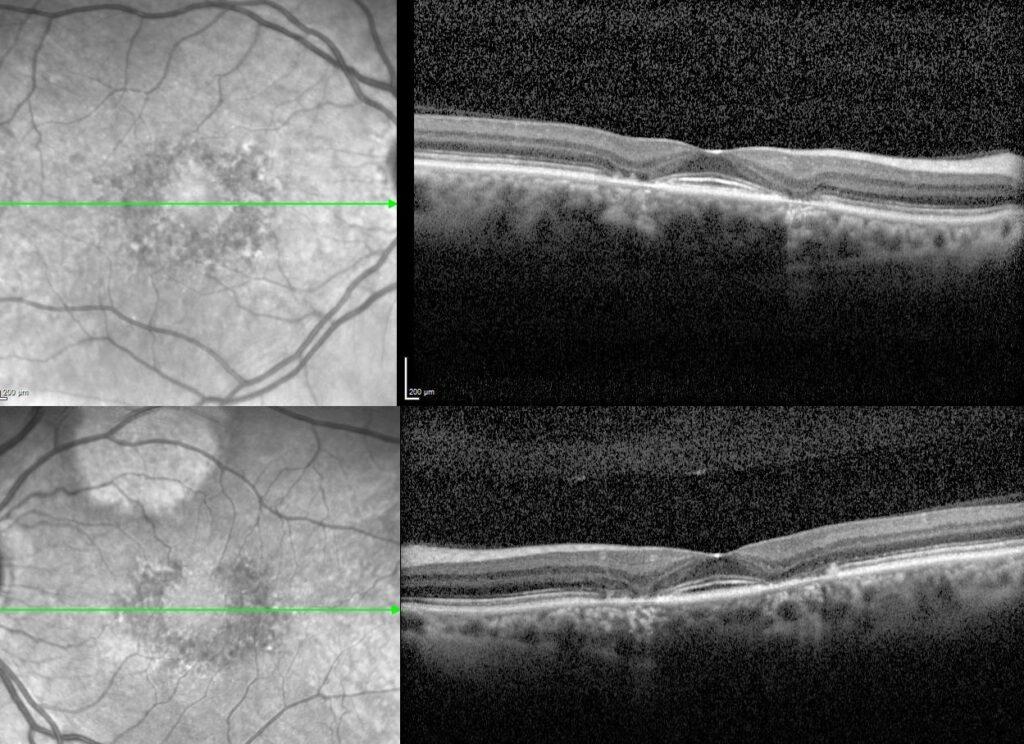
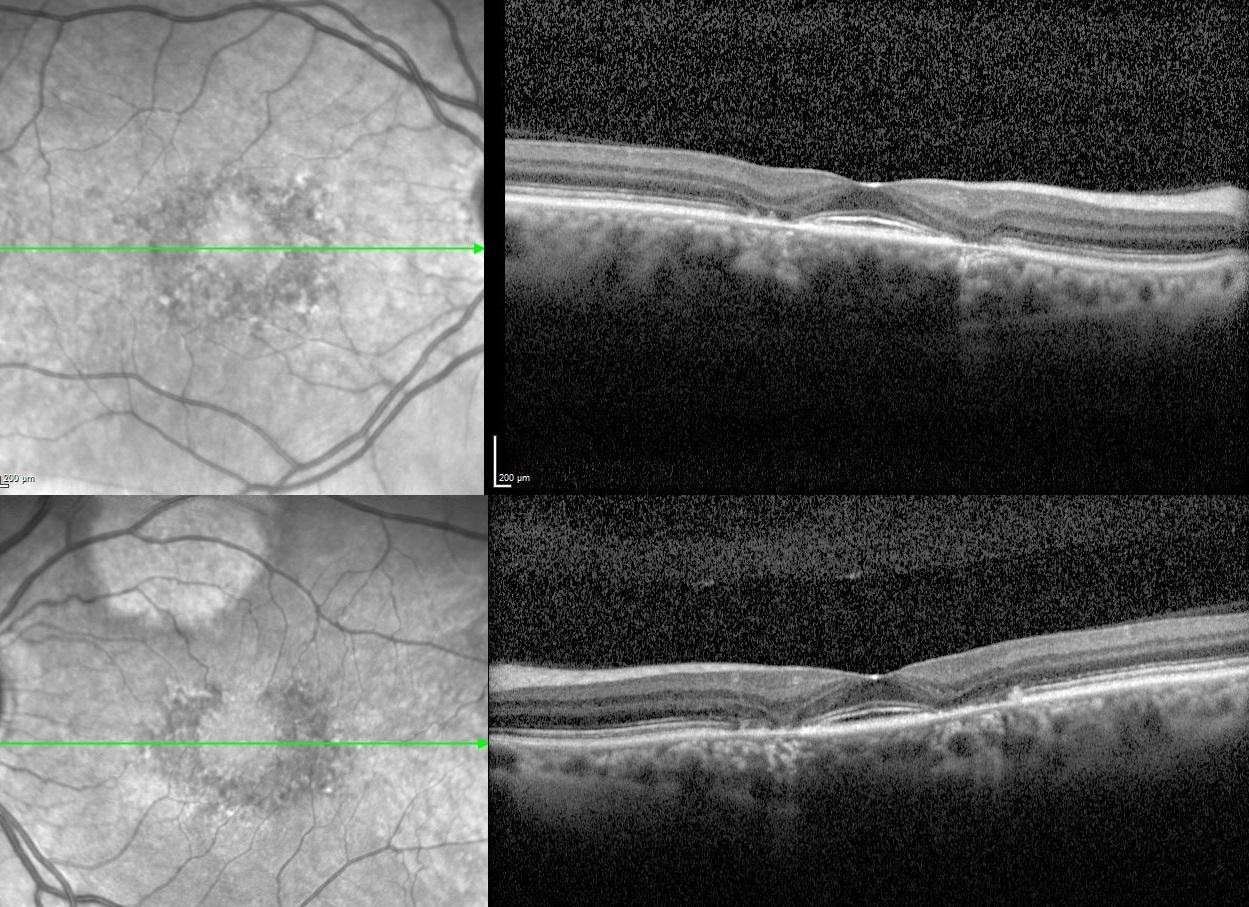
Spectral domain optical coherence tomography demonstrated loss of the elipsoid zone and thinning of the outer retina in the parafoveal region with preservation of these structures in the fovea of both the right and left eyes.
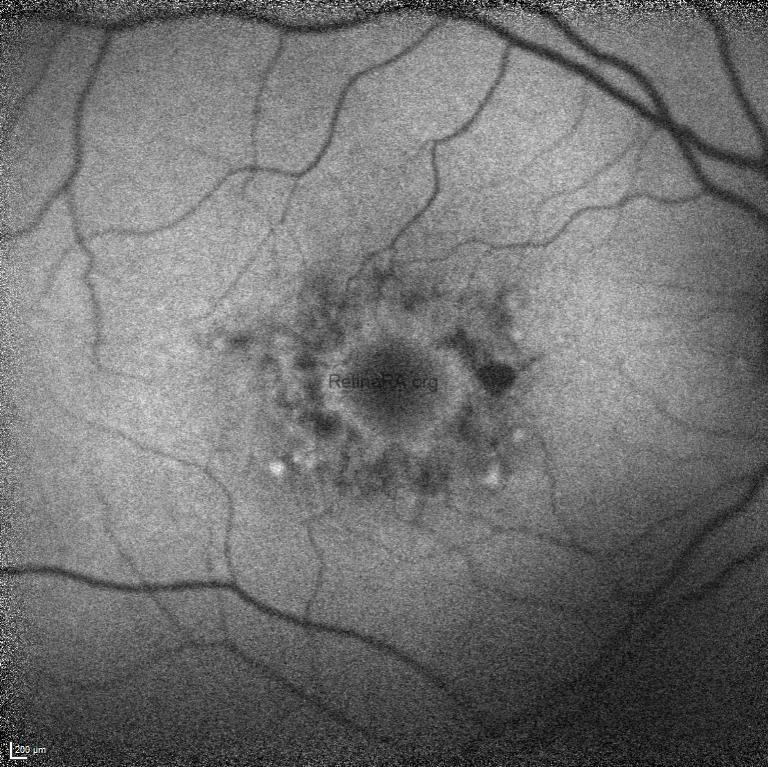
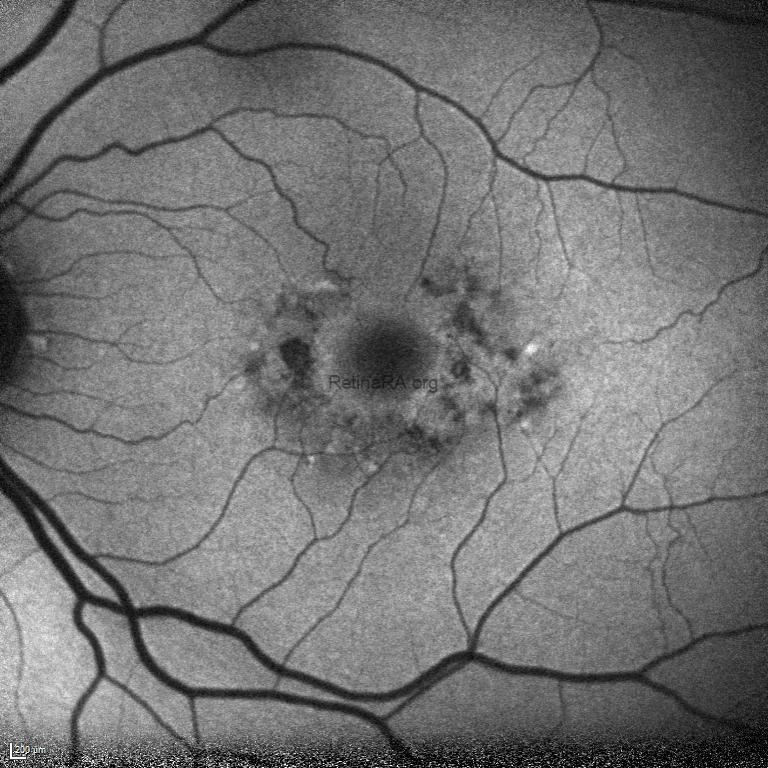
Fundus autofluorescence imaging showed a parafoveal ring of speckled hypoautofluorescence and an external ring of increased signal representing the bull’s-eye macular lesion (parafoveal rings of hypo autofluorescence and hyper autofluorescence).
Retinal toxicity from hydroxychloroquine (HCQ), and its analog, chloroquine, has been recognized for many years. Hydroxychloroquine-induced retinal toxicity is irreversible and can continue to progress following cessation of therapy. It is imperative that patients and clinicians are aware of and monitos for the ocular side effects of this drugs. And before the treatment is initiated with HCQ, a detailed ophthalmic examination should be performed to determine any baseline maculopathy.
HCQ retinopathy causes destruction of macular rods and cones with sparing of foveal cone cells. This pattern provides the typical apperance of bulls-eye maculopathy. High-resolution cross-sectional images of the retina using optical coherence tomography may exhibit distinctive alterations before the development of clinically visible retinopathy. On optical coherence tomography, HCQ retinopathy manifests as disruption, or complete loss of the outer nuclear layer, external limiting membrane, elipsoid zone, and retinal pigment epithelium in the parafoveal region. Usually, there is a preservation of the subfoveal retinal tissue, leading some to believe in the concept of a relative “foveal resistance,” thereby providing many patients with relatively adequate central visual acuity, in spite of advanced perifoveal HCQ retinopathy. This foveal-sparing accounts for the “flying saucer sign” of HCQ retinopathy.
Credit: Kemal Tekin, M.D., from Ulucanlar Eye Training and Research Hospital
Instagram accounts: @retina.academy and @dr.kemaltekin