A 44-year-old female patient presented with complaint of vision loss in her left eye. It has been learnt that she underwent 6 intravitreal injection in her left eye before. The patient had not any systemic disease. The BCVAs were 8/10 in the right eye and 4/10 in the left eye. the refractive errors were -8.00 -1.00 90 D in the right eye and -9.00 -1.25 100 D in the left eye. Intraocular pressures were within normal limits and anterior segment examinations were unremarkable for both eyes.
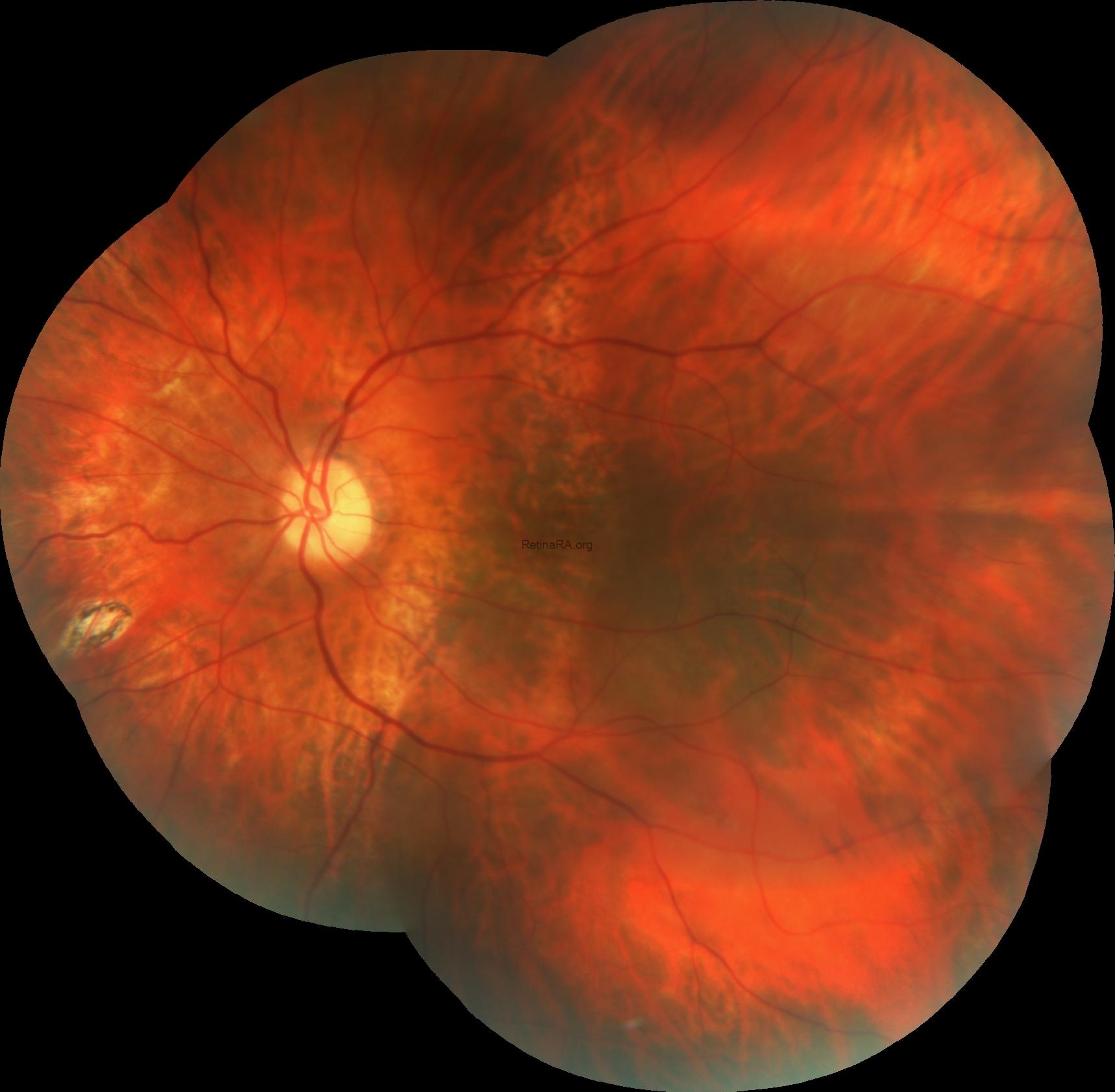
Fundus examination revealed myopic alterations including RPE thinning and attenuation in both eyes win addition to peripapillary atrophy in the right eye.

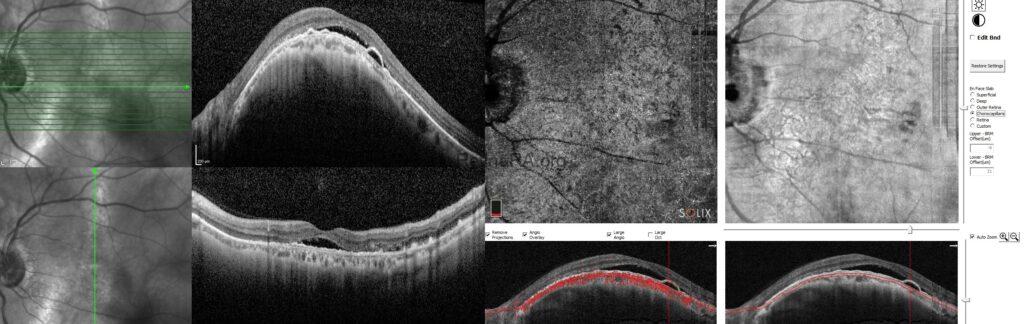
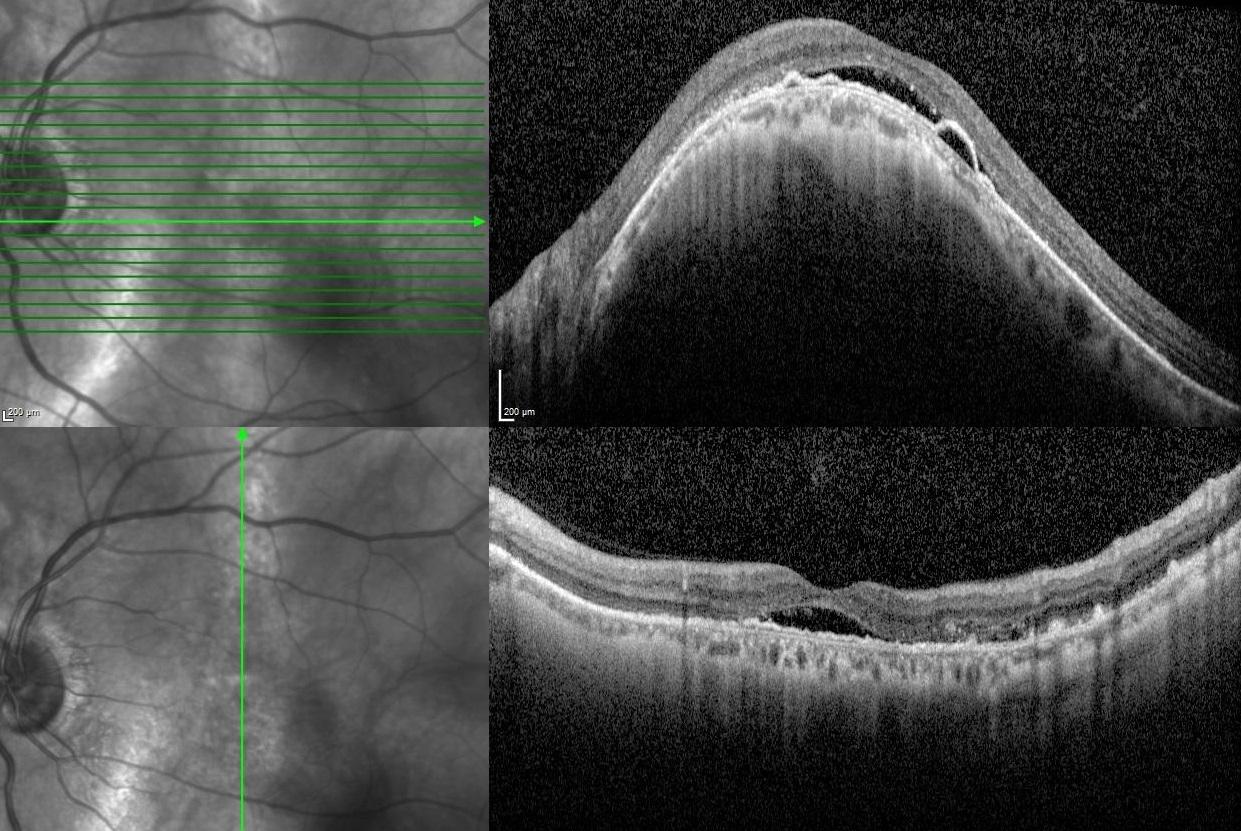
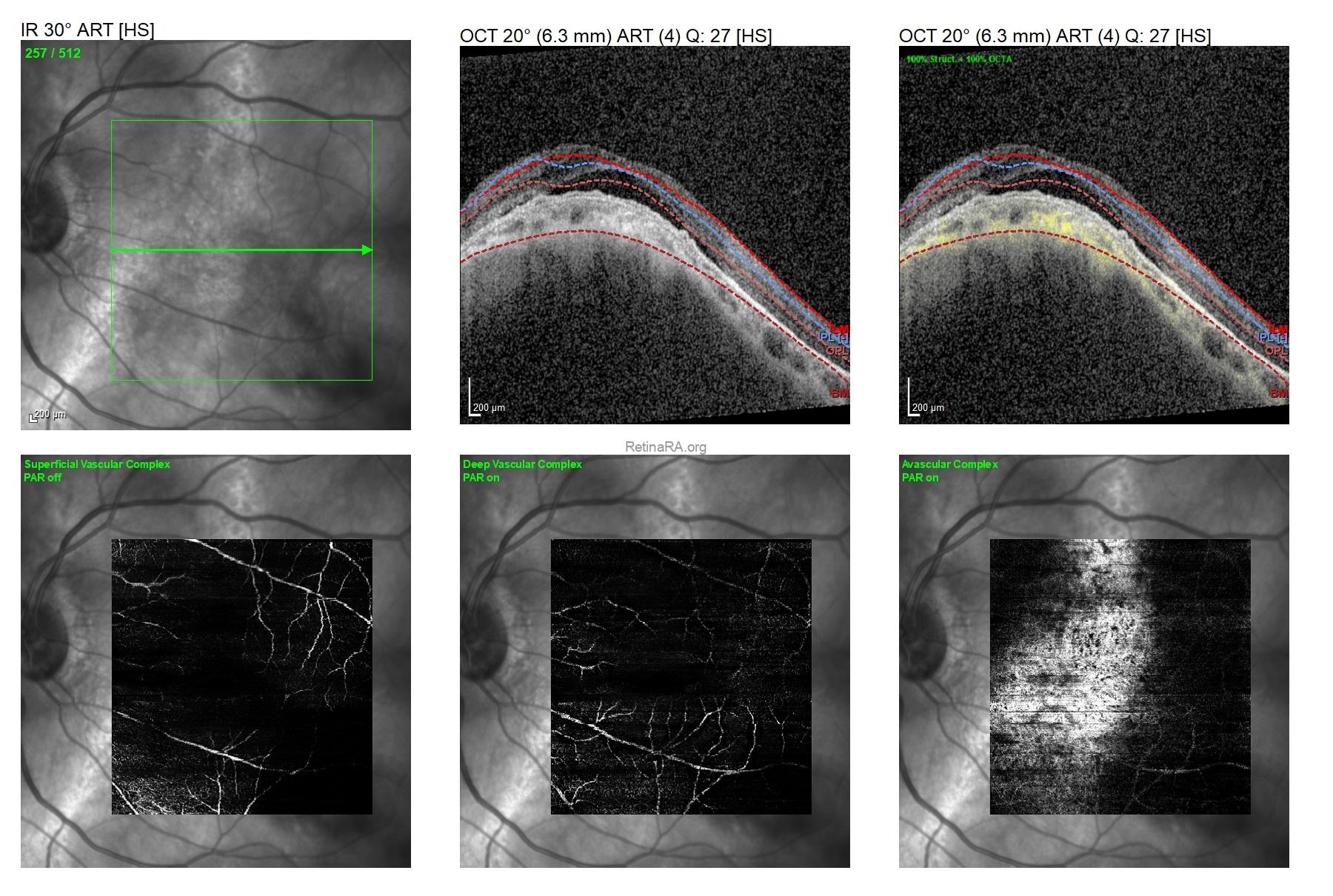
Vertical and horizontal OCT scans of the left eye demonstrated dome-shaped macular configuration with subretinal fluid in addition to shallow pigment epithelial detachment overlying the dome shape.
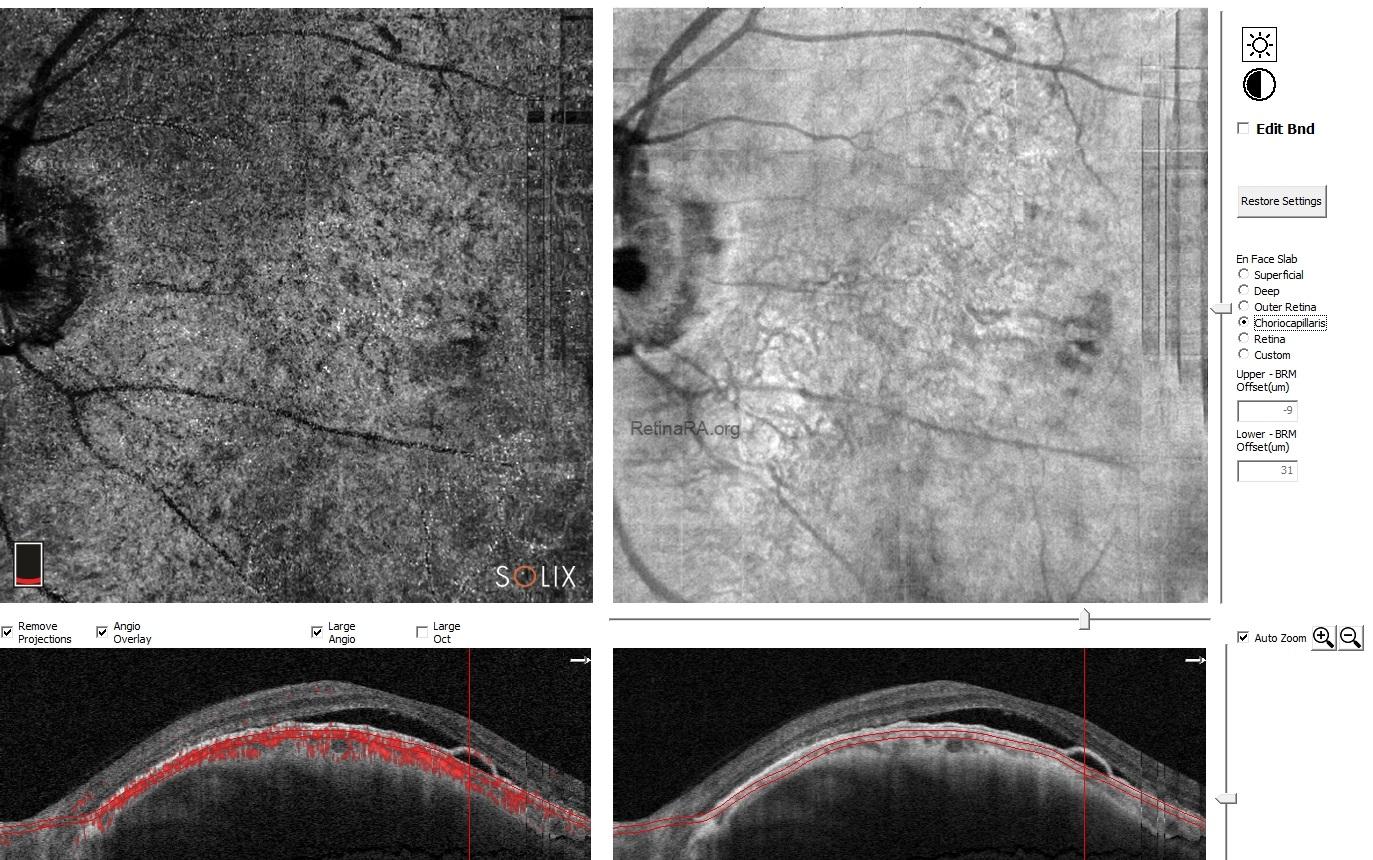
To rule-out the accompanying macular neovascularization, OCT-A was performed and any neovascular membrane could not detected.
Dome-shaped macula (DSM) is characterized by a convex anterior protrusion of the macula associated with high myopia and posterior staphyloma. DSM can be occur in 10-20% of highly myopic eyes. OCT is essential to diagnose DSM and identify the morphological type. Since the dome-shape can appear in different orientations, it is important to obtain both vertical and horizontal scans. The most frequent complication of DSM is serous macular detachment. The prevalence of serous macular detachment in dome-shaped macula has been shown in 2% to 67% of patients with DSM. Shallow irregular PED is another important finding in highly myopic eyes with DSM. It can be associated with serous macular detachment in the absence of macular neovascularization. This finding is in contrast to the frequent association of shallow irregular PED with macular neovascularization in conditions such as central serous chorioretinopathy.
Credit: Kemal Tekin, M.D., from Ulucanlar Eye Training and Research Hospital
Instagram accounts: @retina.academy and @dr.kemaltekin