This was a 33 year-old male without known any systemic or ocular disease applied to clinic with blurred vision in his left eye. In his medical history, there was no recent or chronic drug use. The BCVAs were 20/20 for the right and 20/32 for the left eyes. IOPs were within normal limits and anterior segment examination was unremerkable.
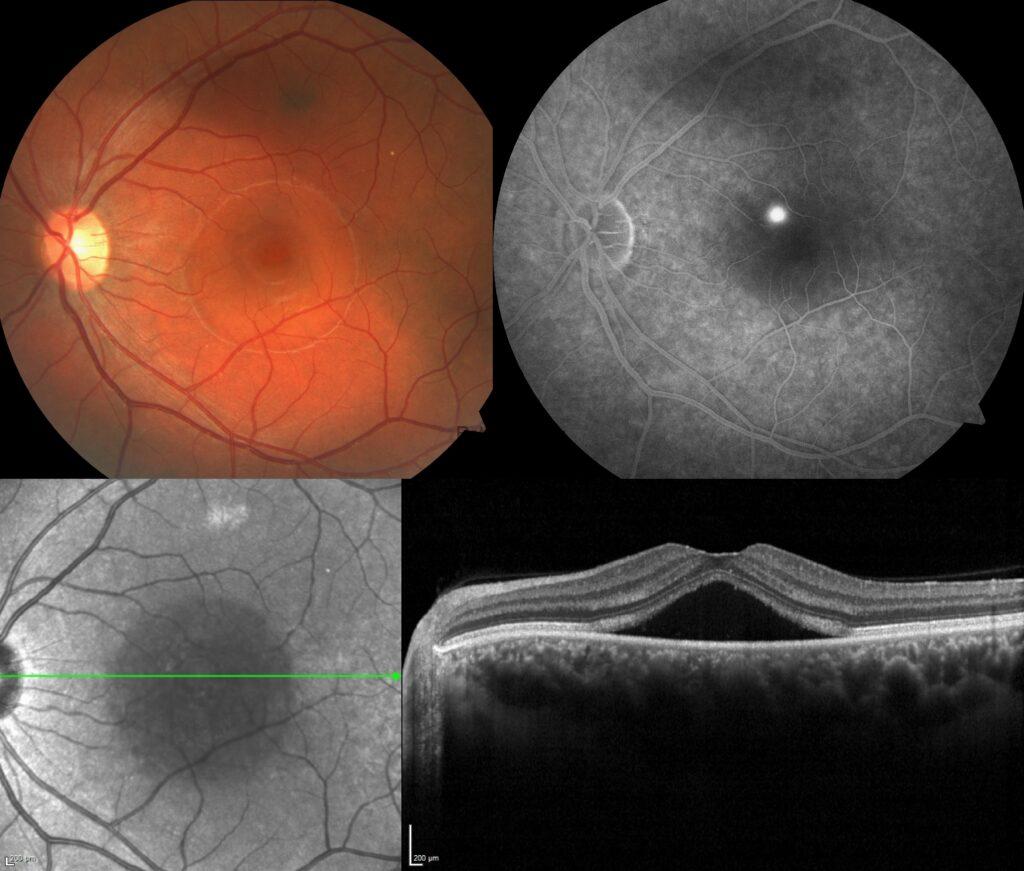
Fundus images of the left eye showed the abnormal foveal reflex with an area of retinal elevation consistent with subretinal fluid in the central retina. Additionally, a choroidal nevus located superior of the fovea was also noted. The right was completely normal.


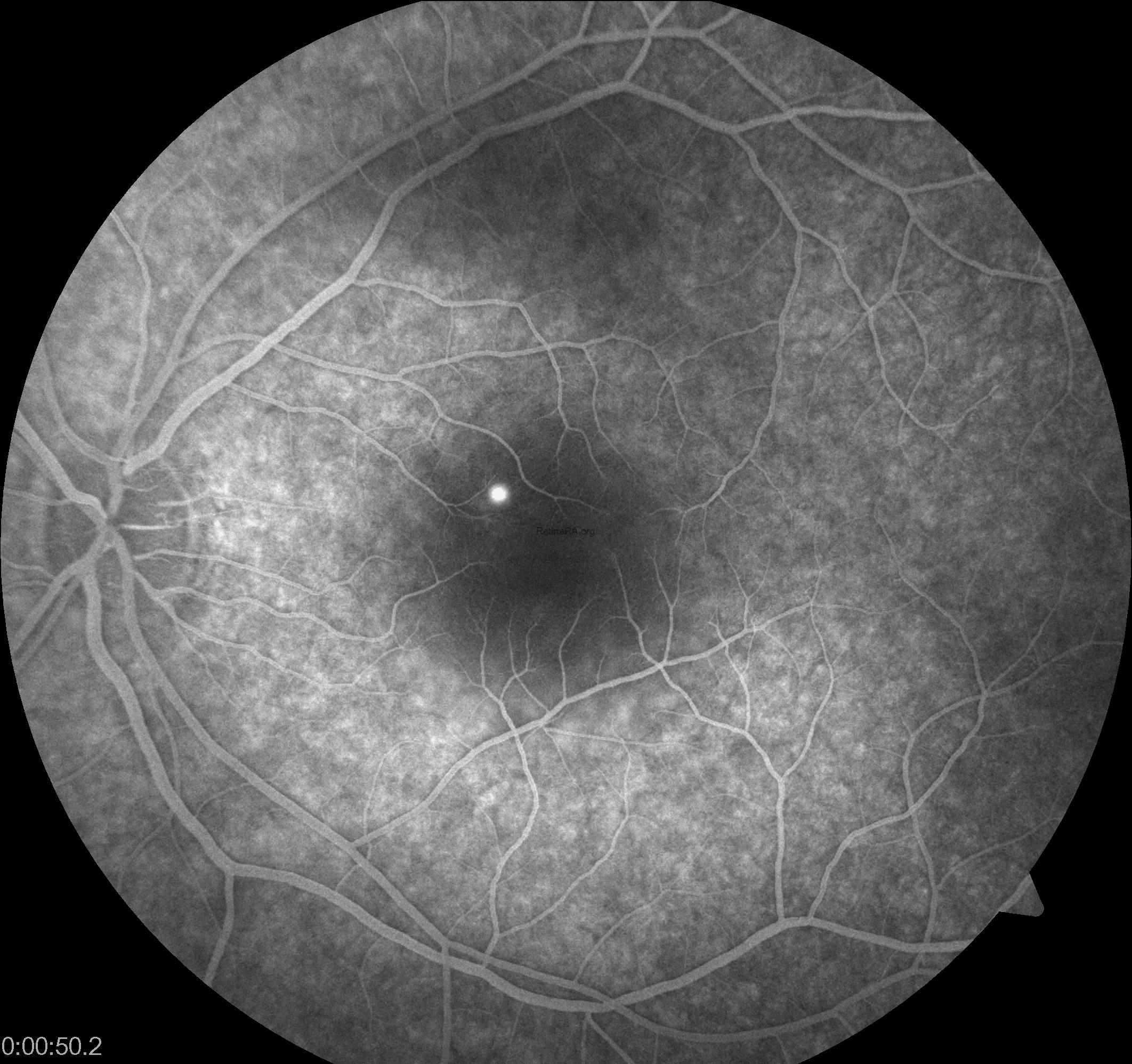
On fundus fluorescein angiography, a small focal hyperfluorescent leak that appears early and increases in size and intensity as the angiogram progresses called as inkblot appearance was seen in the affected eye.


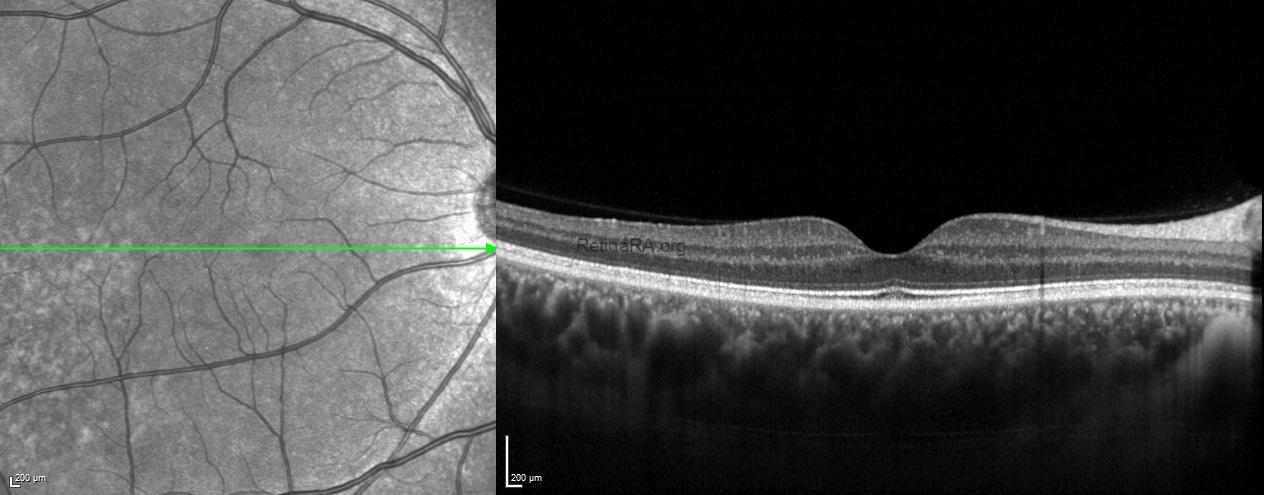
Enhanced depth imaging spectral domain optical coherecence tomography scans exhibited choroidal thickening bilaterally in addition to serous macular detachment in the left eye.
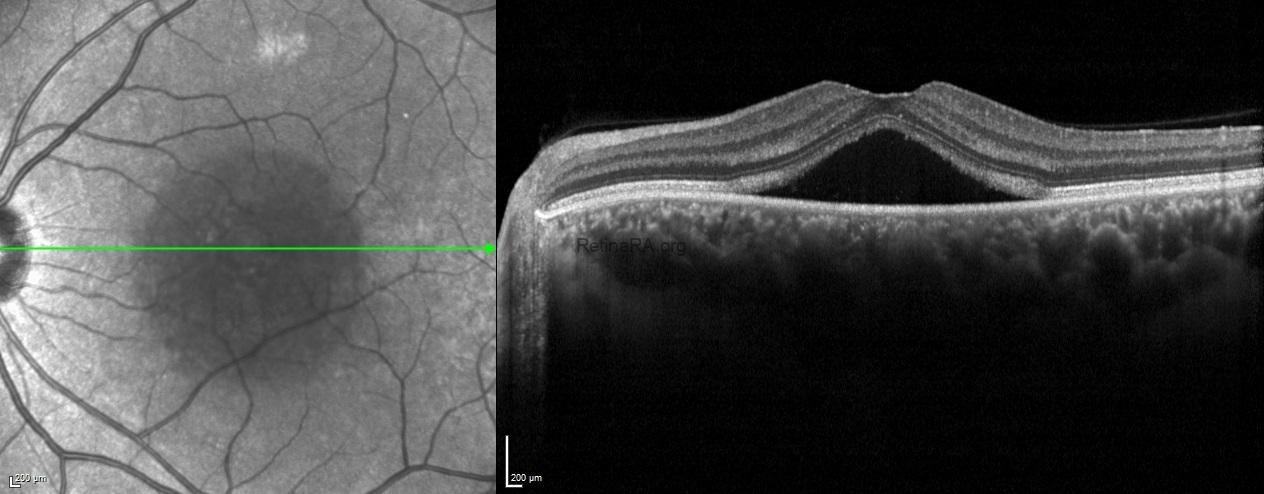
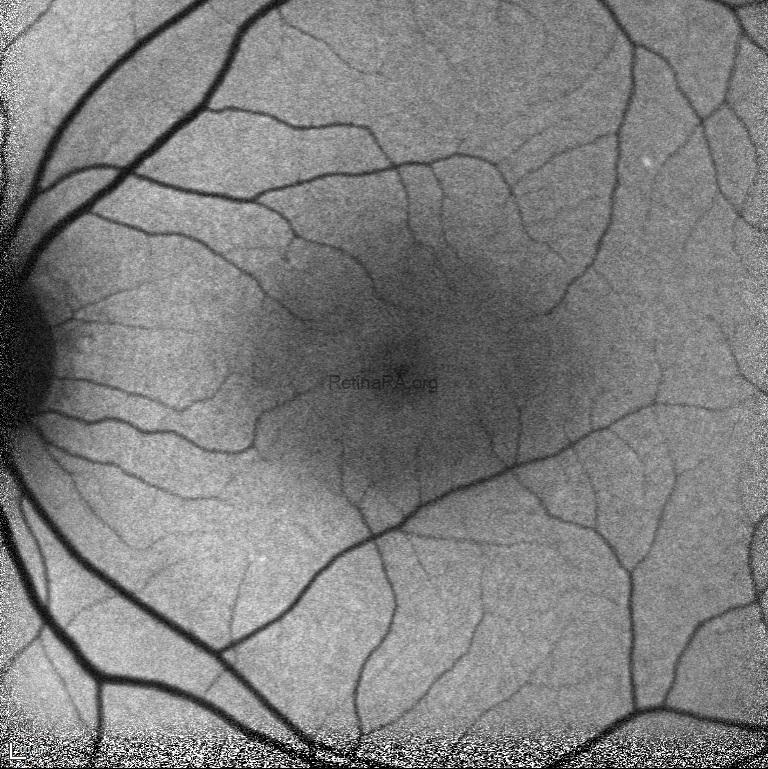
Fundus autofluorescence demonstrated hypoautofluorescence of the central macula due to the subretinal fluid in the left eye.
According to these multimodal imaging characteristics, the patient was diagnosed with central serous chorioretinopathy and informed that his visual changes were likely to improve without intervention.
Central serous chorioretinopathy (CSCR) is characterized by serous retinal detachments frequently involving the macula and usually associated with focal pigment epithelial detachments, choroidal hyperpermeability, and increased choroidal thickness. It is commonly seen in young to midde-aged men and may be associated with type A personality and corticosteroid usage. Most cases resolve spontaneously, but chronic or recurrent forms can lead to permenant visual impairment.