
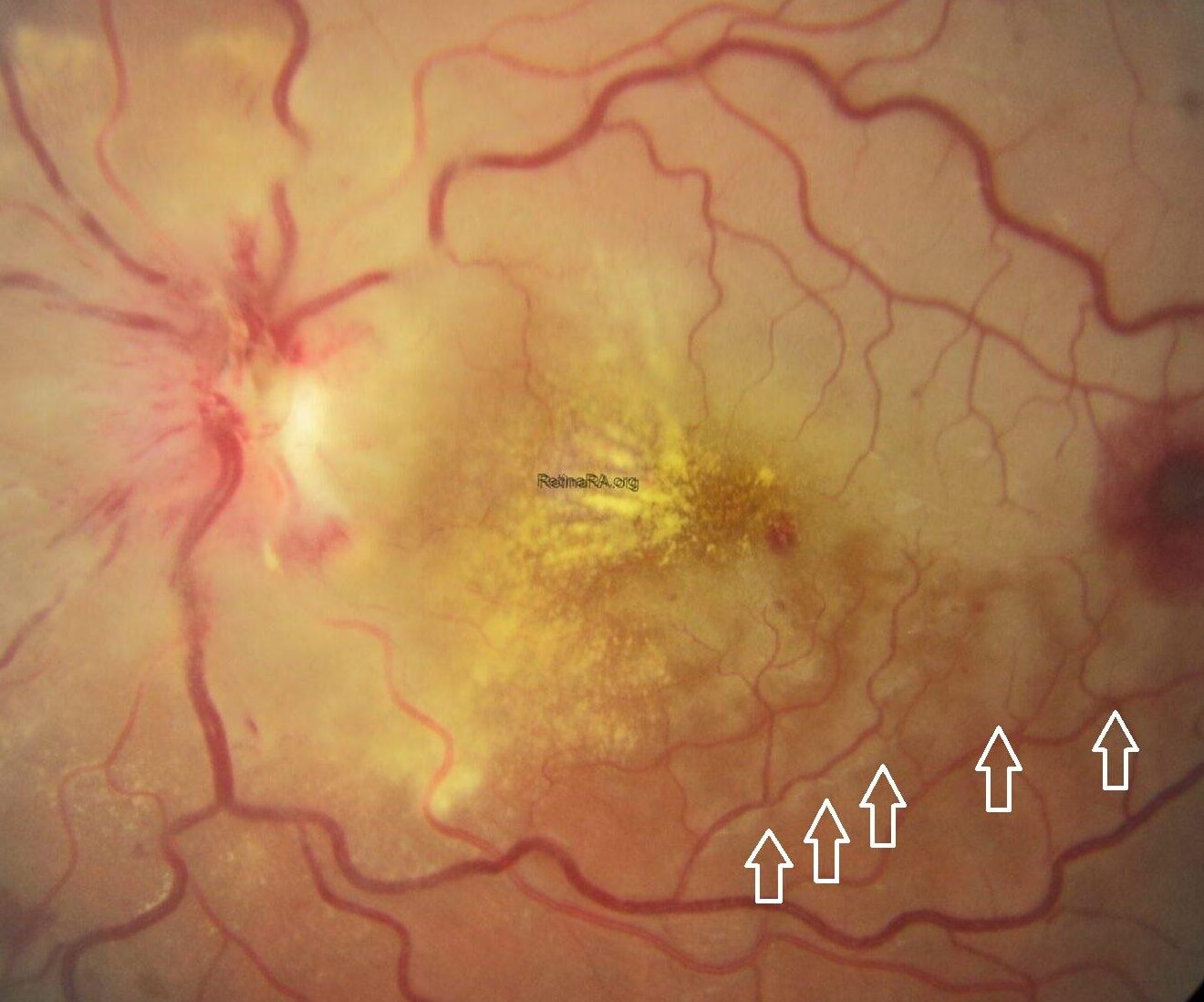
A patient presented with a complaint of sudden loss of vision in the right eye. Fundoscopic examination revealed mild venous dilatation and tortuosity, optic disc edema, flame-shaped retinal hemorrhages around the disc, cotton-wool spots (soft exudates) in the nasal quadrant, and lipid exudates (hard exudates) forming a macular star pattern around the fovea. Additionally, the superior temporal quadrant of the retina was noticeably pale, and there was mild paleness around the inferior temporal branches of the retinal vein (white arrows).
The infectious disease panel, including Bartonella henselae, Treponema pallidum (syphilis), Borrelia burgdorferi (Lyme disease), and TORCH serologies, was negative. The patient’s systemic blood pressure was 110/80 mmHg, and no hypertension was detected during follow-up. Rheumatologic evaluation demonstrated anti-cardiolipin antibody positivity, and the patient was referred to rheumatology, where a diagnosis of systemic lupus erythematosus (SLE) was established.
Based on the clinical findings, the patient was diagnosed with SLE-associated neuroretinitis (stellar) and BRAO. The pallor around the inferior temporal vein branches was interpreted as perivenular fern-like PAMM (white arrows). Furthermore, the presence of venous dilatation, vascular tortuosity, and perivenular fern-like PAMM suggested that, although the patient did not have complete CRVO, there may have been a partial occlusion of the central retinal vein due to optic nerve head stasis.
It was concluded that the coexistence of neuroretinitis, BRAO, and PAMM was secondary to SLE-associated thrombotic tendency and vasculitis. Compared with diabetic retinopathy and hypertensive retinopathy, the more occlusive nature of SLE retinopathy generally leads to more profound ischemia.
Neuroretinitis is not considered a common cause of vision loss in SLE; moreover, it has been reported very rarely as a presenting feature of SLE. Neuroretinitis is defined as an inflammatory condition of the retina and optic nerve. Its pathophysiology involves optic disc edema that begins 1-3 weeks before the appearance of the stellate macula and resolves spontaneously after 8-12 weeks. Leakage of lipoproteinaceous material from optic disc vessels and its deposition in the outer retinal layers are responsible for optic disc swelling. The swelling subsides within weeks, leaving radial lipoprotein deposits in the plexiform layer of the retina. However, the exact pathogenesis behind neuroretinitis in SLE is unknown. The sudden onset of unilateral painless visual loss is the typical clinical presentation of neuroretinitis in these patients.

Credit: Trakya University Ophthalmology Clinic
Instagram account: @ophthagram.thrace
Editing: M. Giray Ersoz, MD, FEBO
Biruni University School of Medicine, Department of Ophthalmology, Istanbul, Turkey
Instagram accounts: @retina.review and @retina.dr.girayersoz
