A 57-year-old woman was referred from the endocrinology department for evaluation of diabetic retinopathy. She had a history of hypertension and poorly controlled diabetes mellitus. Approximately 10 years earlier, she had undergone laser treatment for macular edema. Best-corrected visual acuity was 0.8 in both eyes, and intraocular pressures were within normal limits.
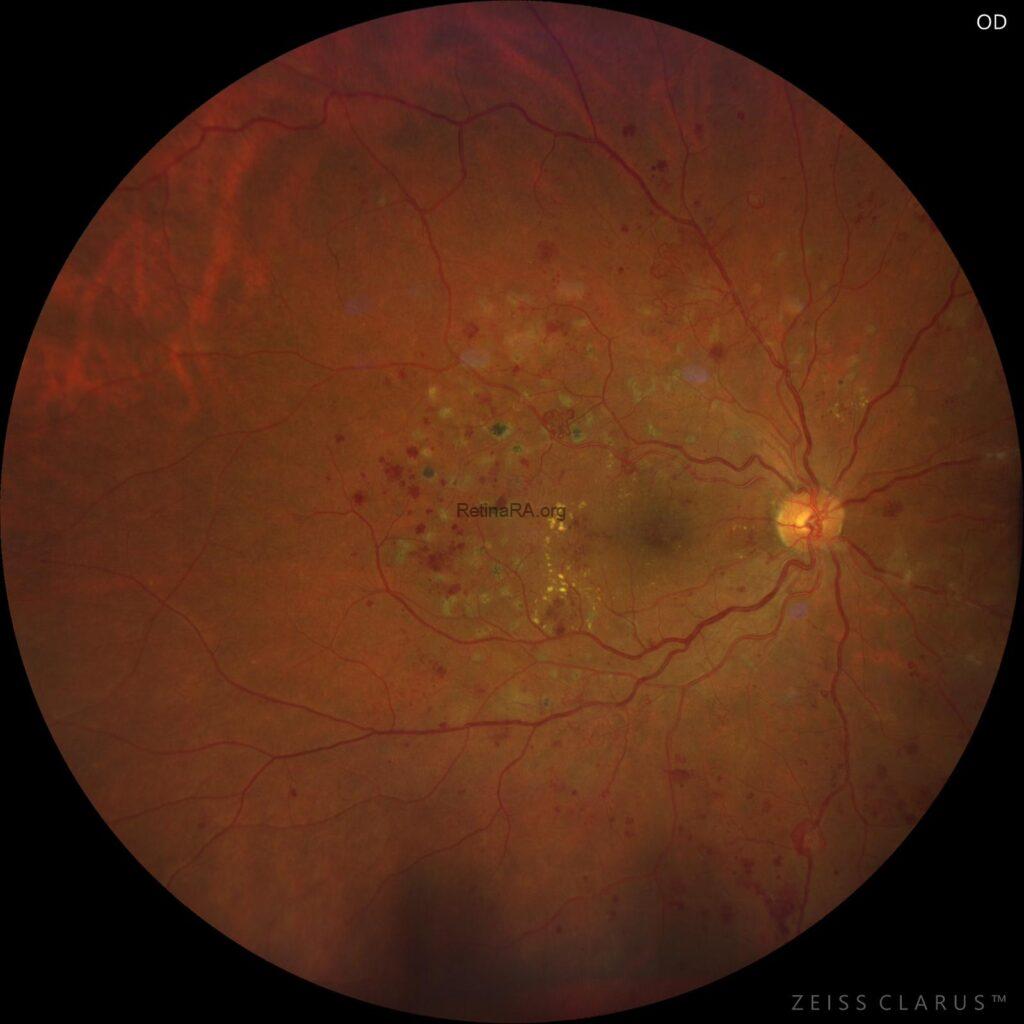
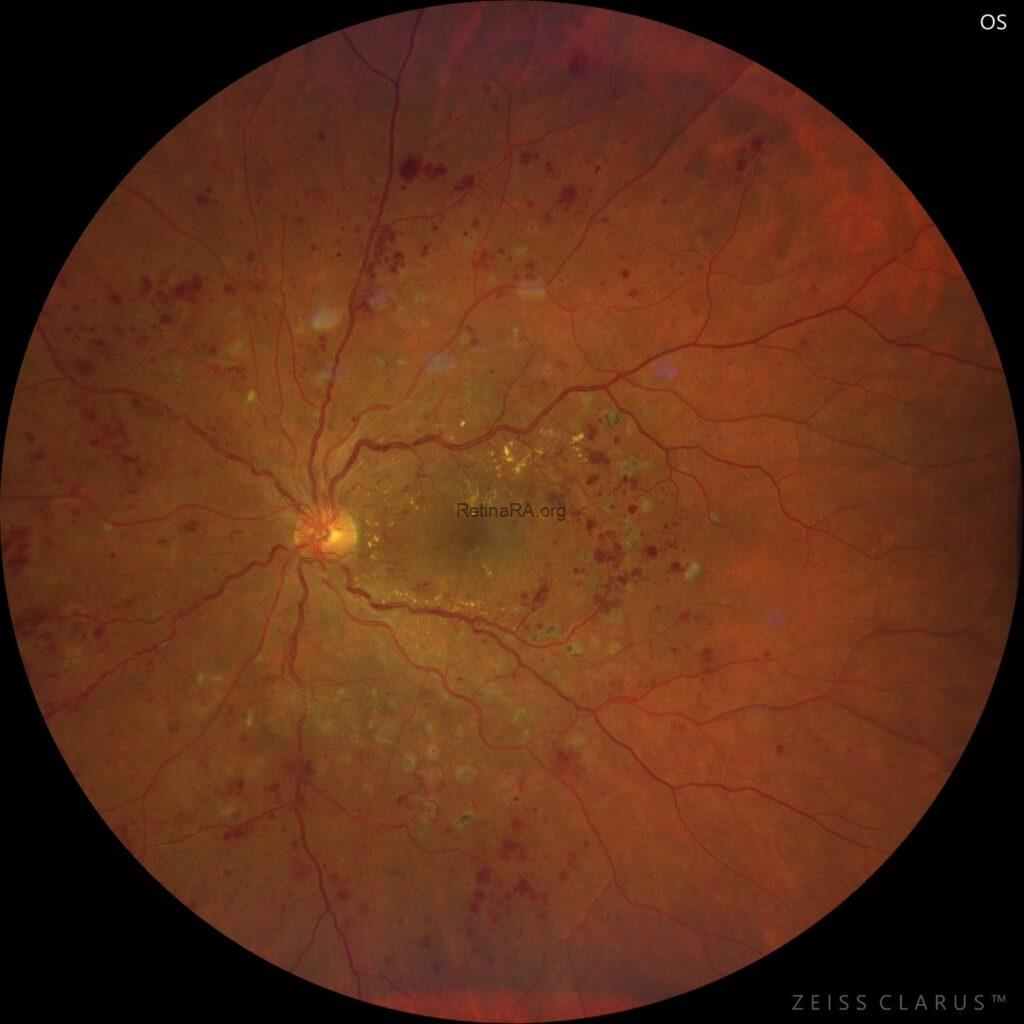
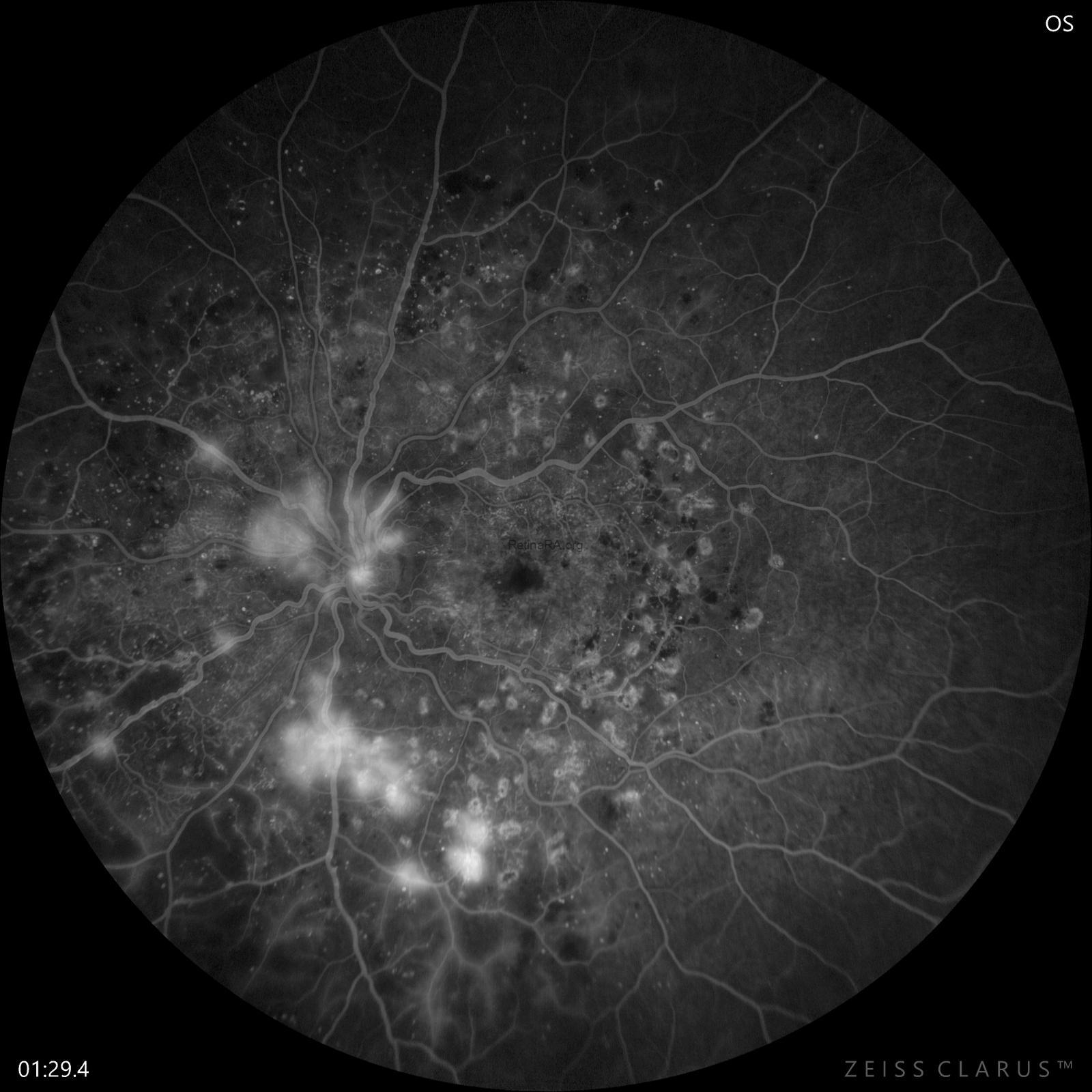
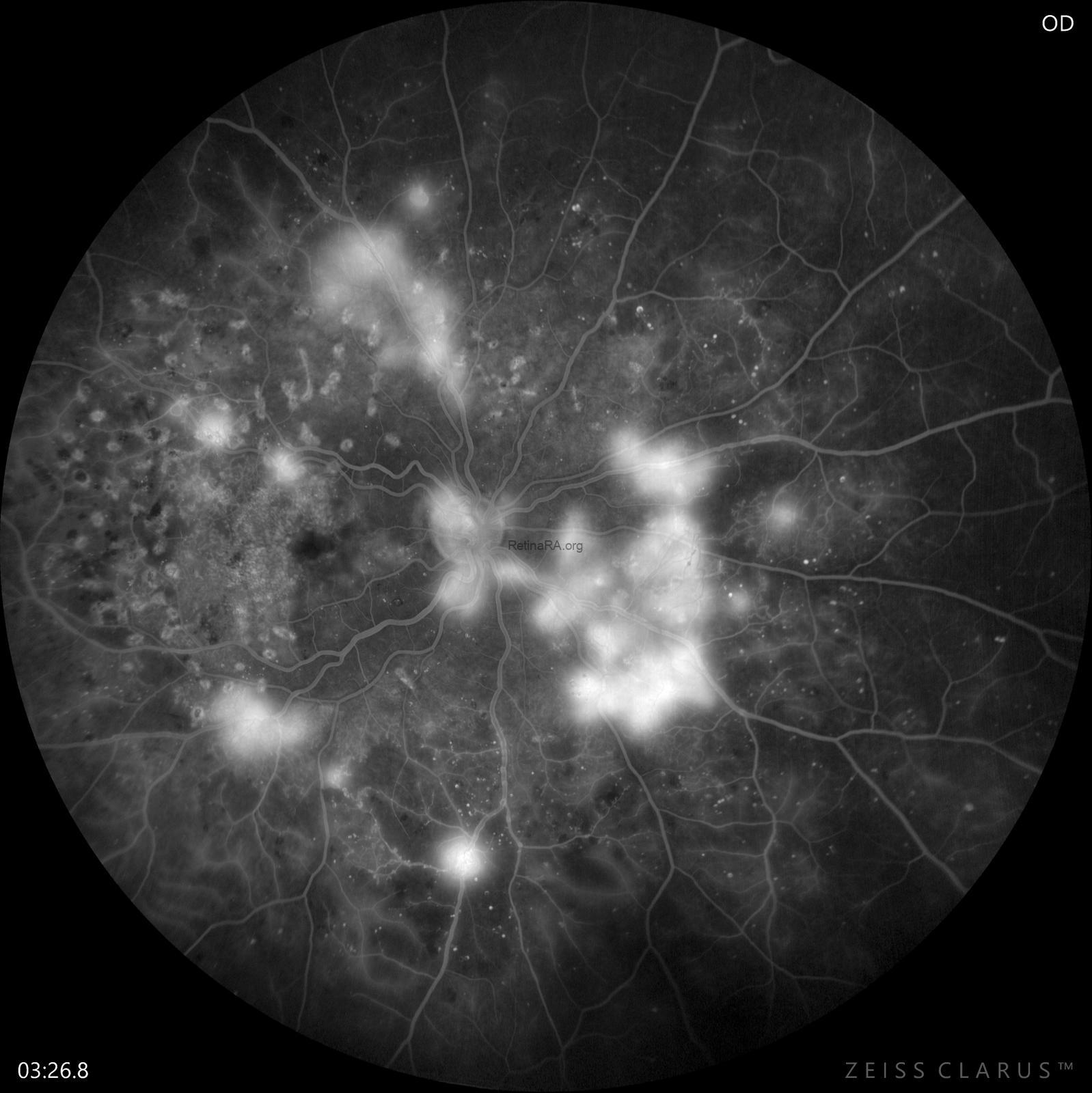
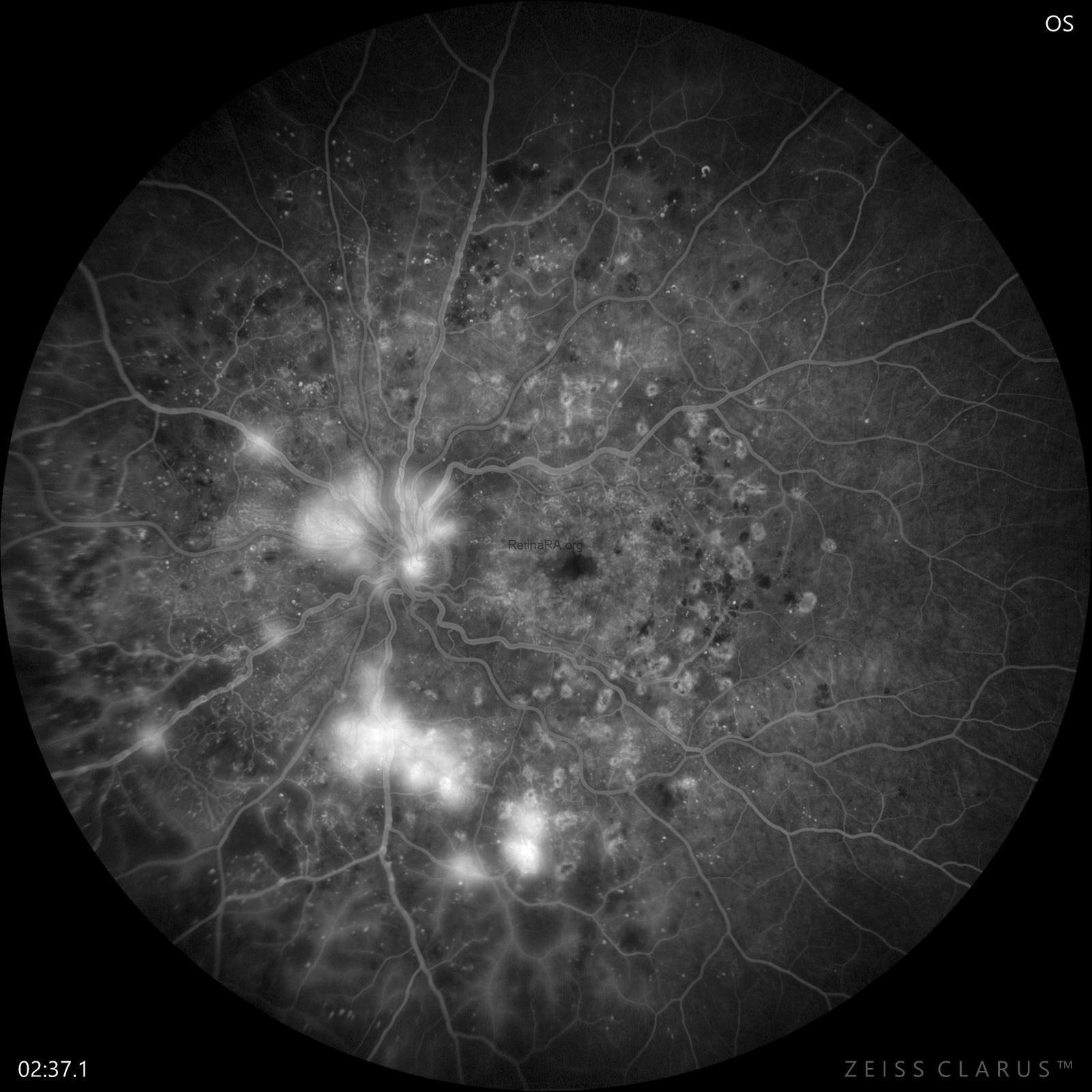
Fundus examination revealed previous focal macular laser scars, widespread macular microaneurysms, hard exudates, venous omega loops, in additon to retinal and optic disc neovascularization in both eyes.
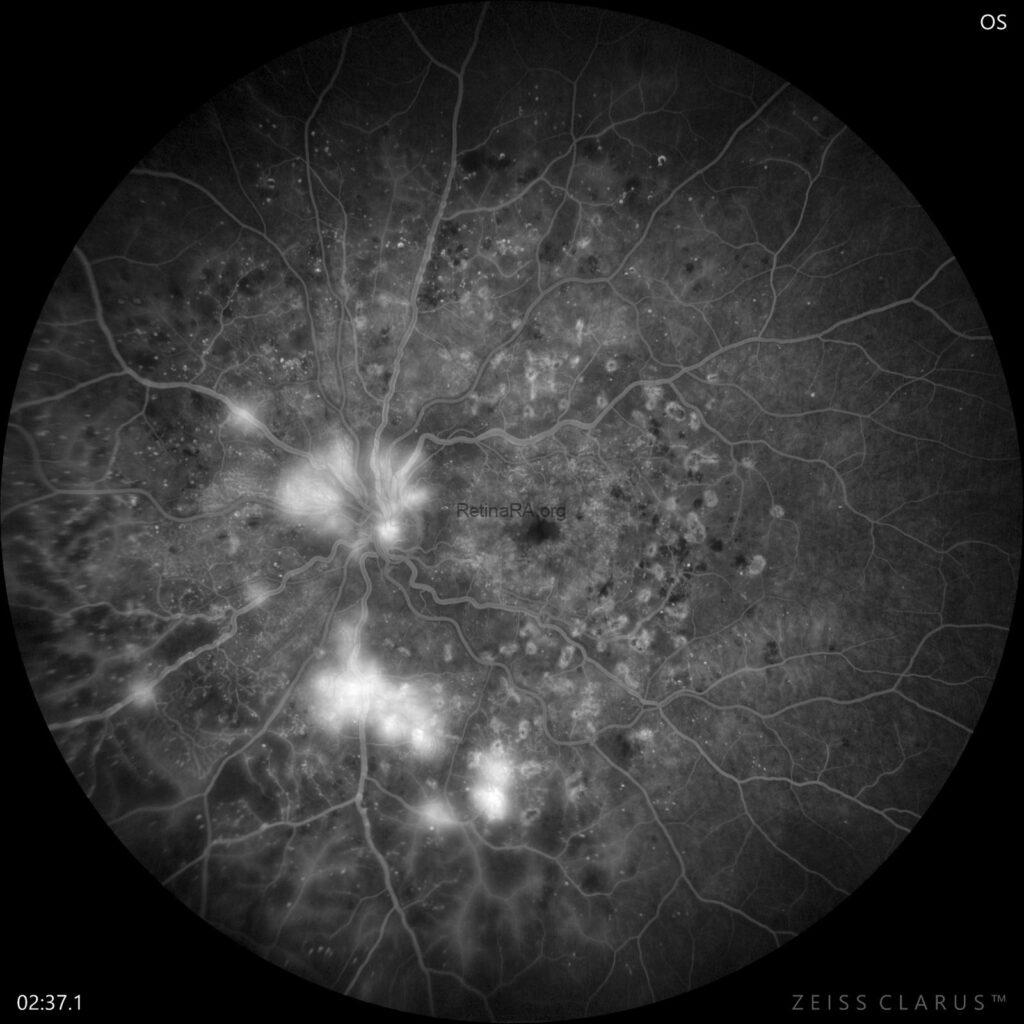
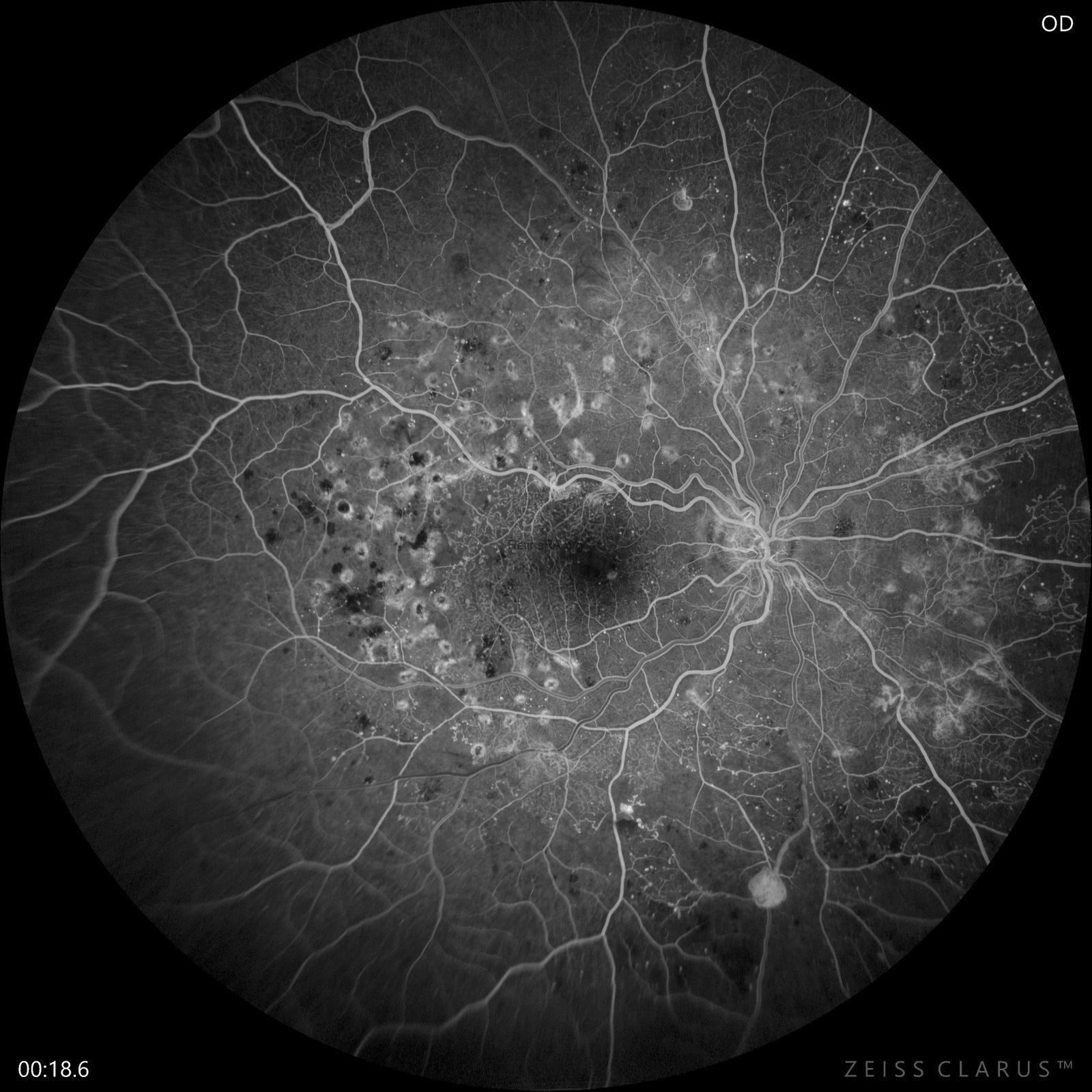
Early and late phases of fundus fluorescein angiography demonstrated pinpoint hyperfluorescent leakage corresponding to microaneurysms, vascular loops, and venous beading, as well as macular and peripheral areas of nonperfusion in both eyes. In addition, there was leakage from retinal and optic disc neovascularization.
Proliferative diabetic retinopathy (PDR) represents the most advanced and vision-threatening stage of diabetic retinopathy. PDR is the most serious complication of diabetic retinopathy and can lead to vision loss. It is characterised by the presence of abnormal new blood vessels, either on or within one disc diameter of the optic disc (NVD) or elsewhere in the retina (NVE). High-risk PDR is characterized by NVD greater than one-fourth to one-third disc area in size; any NVD with a vitreous or preretinal hemorrhage; or NVE greater than one-half a disc area in size with a vitreous or preretinal hemorrhage. In severe cases, fibrovascular membranes grow over the retinal surface and tractional retinal detachment with sight loss can occur, despite treatment. Early detection and timely intervention with panretinal photocoagulation, intravitreal anti-VEGF therapy, and vitreoretinal surgery remain essential to prevent irreversible vision loss.
Credit: Kemal Tekin, M.D., from Ulucanlar Eye Training and Research Hospital
Instagram accounts: @retina.academy and @dr.kemaltekin