
A 27-year old female patient was referred to our attention because of unspecified “bilateral juvenile maculopathy with drusen in OU” found during a routine ophtalmological checkup. Patient was asymptomatic, with no complains of reduced central vision and/or metamorphopsia, and first received her diagnosis when she was 16 years-old.
Her BCVA was 20/20 OU, her IOP was normal (17 mmHg OU) and anterior segment examination was unremarkable in both eyes.
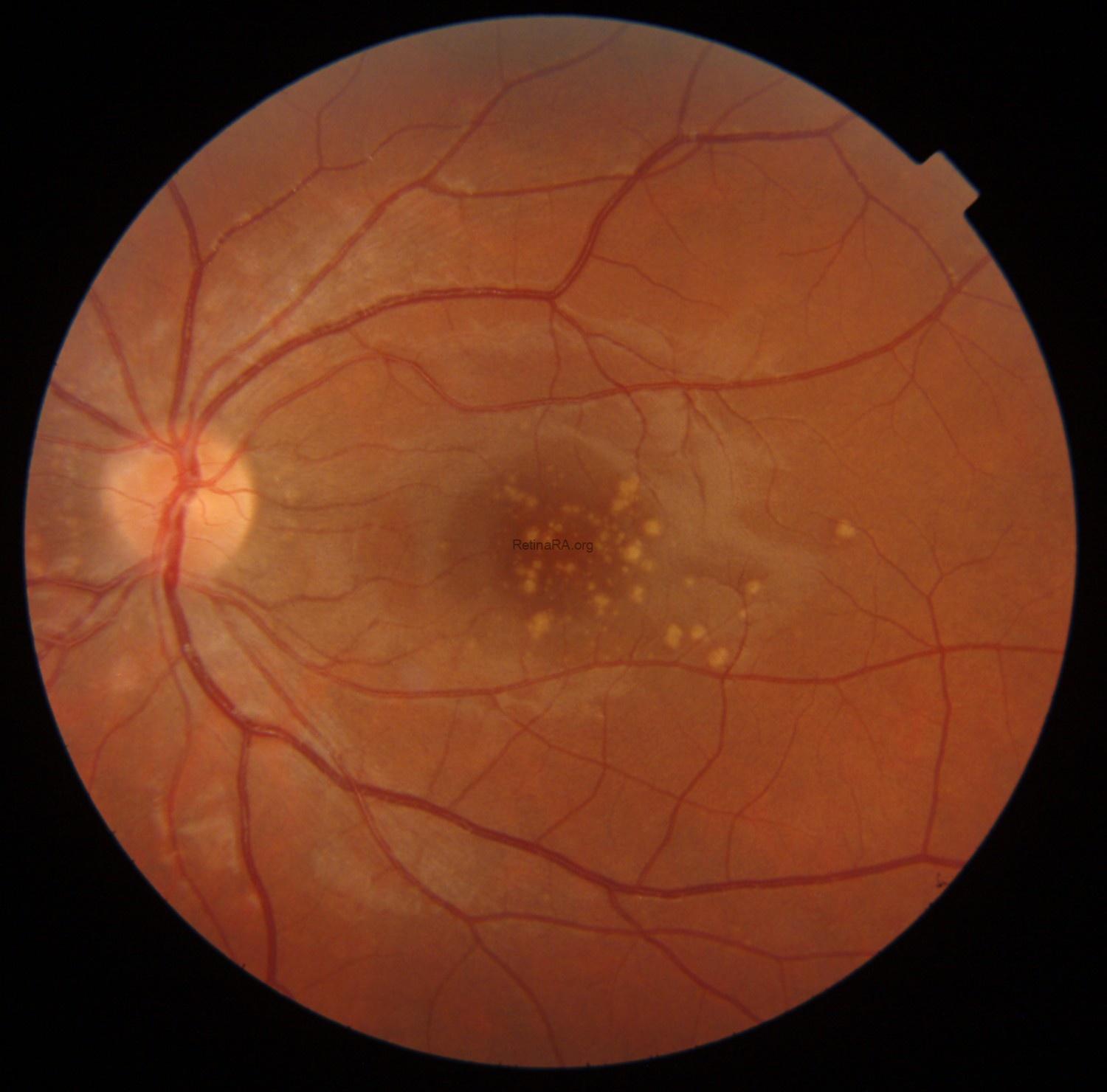
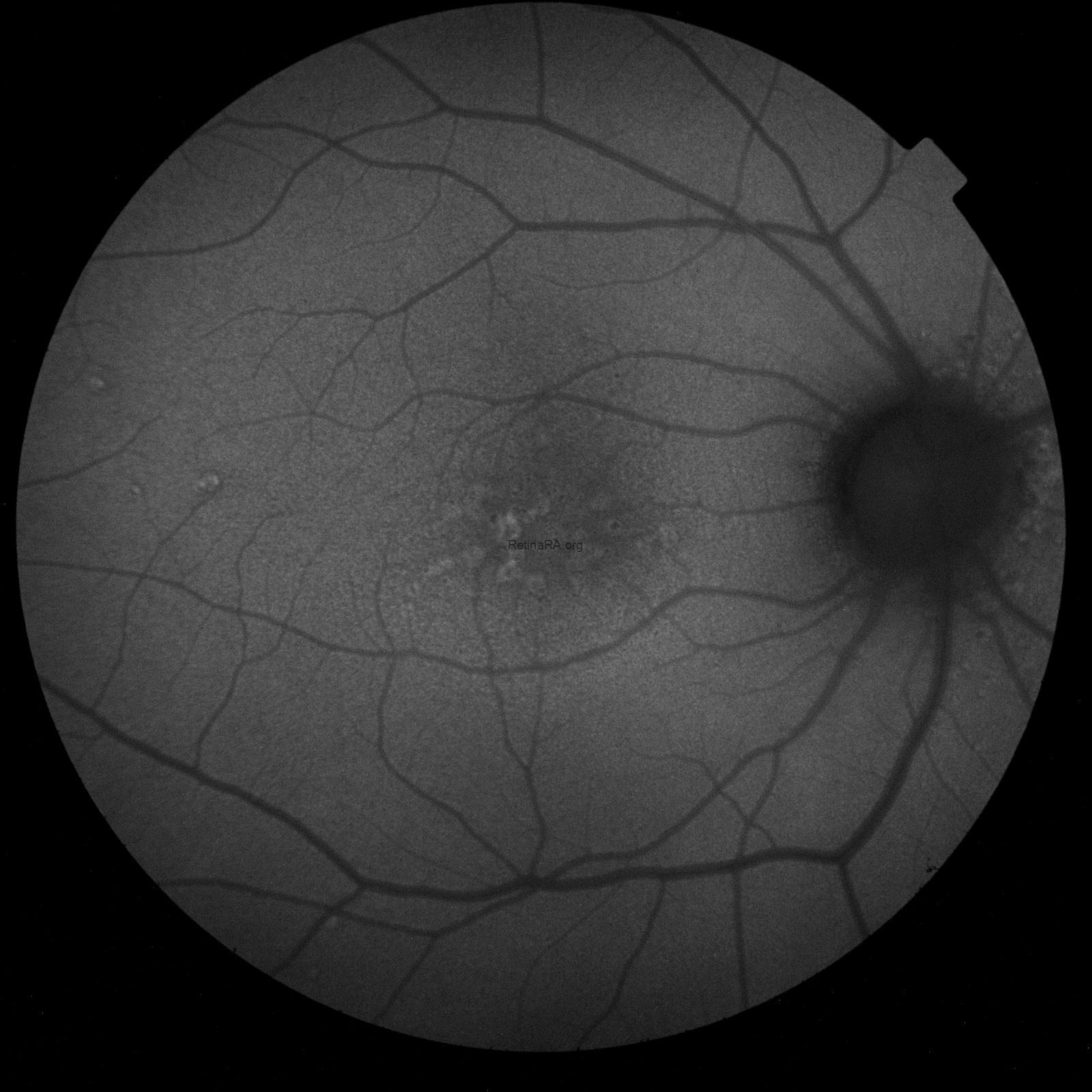
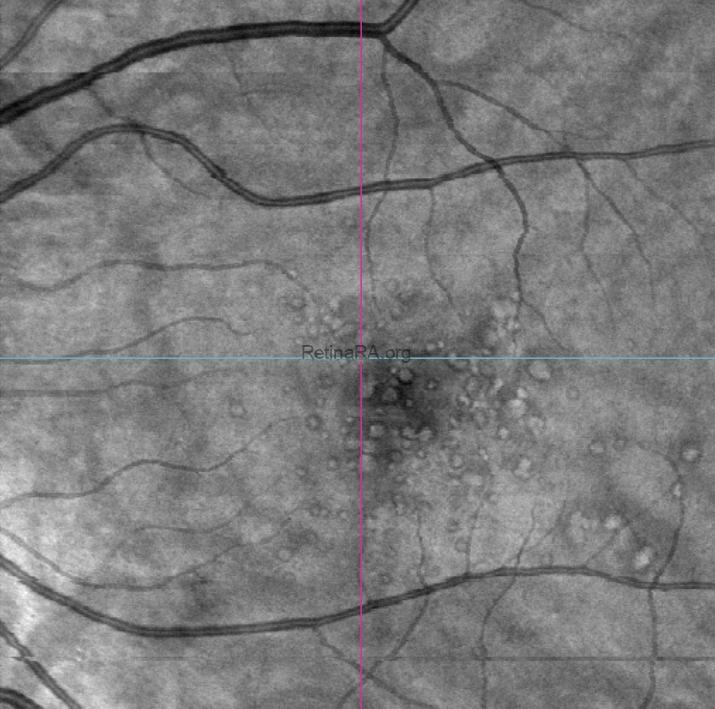
Fundus true-color photo shows multiple large yellowish drusen-like lesions scattered throughout the posterior pole and mainly clustered in the macular region in OU. On FAF, these lesions appear hyperautofluorescent with a surrounding hypoautofluorescent halo.


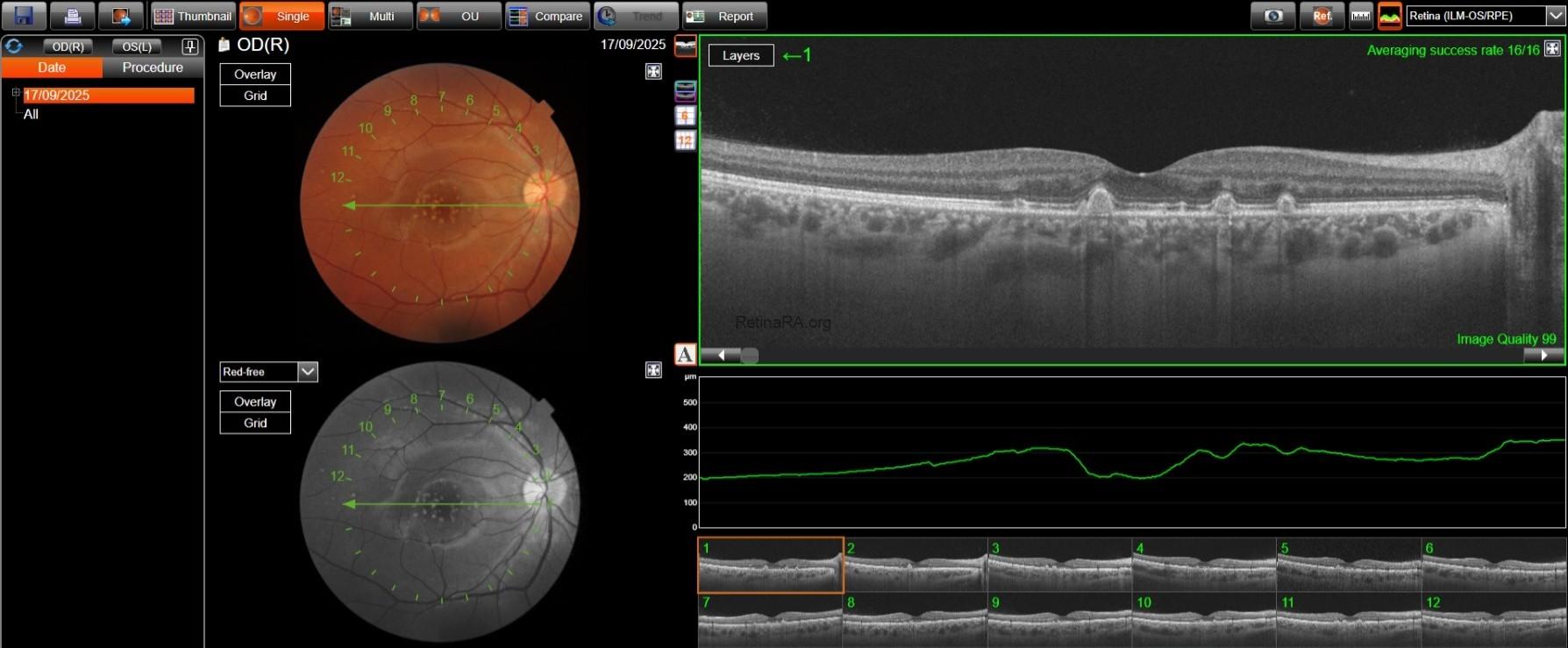
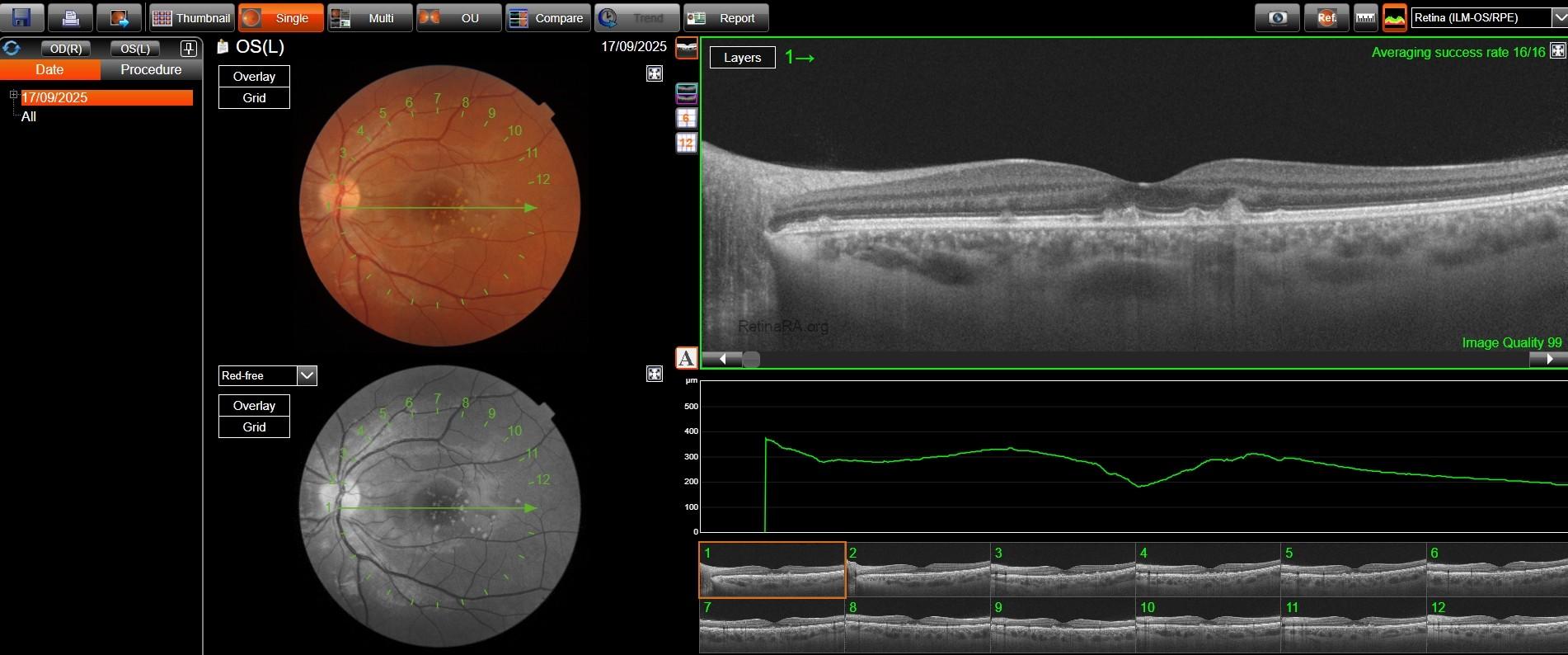
SD-OCT reveals dome-shaped RPE elevations with internal homogeneous medium reflectivity and increased central backscattering compared to their periphery; their size is variable, with the largest ones even deforming the overlying EZ band and possibly thinning the overlying retinal layers. No RPE and/or outer layer atrophy was found, as well as no subretinal and/or intraretinal fluid. OCT-A was unremarkable OU. En-face OCT segmented shows an hyperreflective center surrounded by a marked hyporeflective ring.

The patient already had an OCT performed in 2023, which showed complete stability of the lesions in both number and size.
A diagnosis of Large Colloid Drusen was made based on patient history, absence of relevant symptoms, and retinal imaging.
Large Colloid Drusen (LCDs) represent a specific type of early-onset drusen (EODs), along with cuticular drusen (CDs) and Malattia Leventinese, also known as Doyne Honeycomb Retinal Dystrophy. LCDs were first described by Guigui et al. in 2011: the medium age of onset is reported to be 35, and they are found more frequently in females than men. LCDs are usually asymptomatic and are often first found ona fundus exam during a routine check-up.
On fundus examination, LCDs appear as large yellowish drusen-like lesions scattered throughout the posterior pole. SD-OCT is able to better show their main features as large dome-shaped RPE elevations (usually larger than 200 microns, with a mean diameter of about 400 microns), with a base-to-height ratio of about 1 and with homogeneous medium reflectivity; several reports have however highlighted a possible difference in reflectivity between LCDs center and periphery, with the latter being relatively hyporeflective, as well as a relatively marked central backscattering as opposed to the periphery. This difference could be attributed to either a different composition of LCDs in their center as opposed to their periphery, a different incidence of the beacon on the periphery, or both. Interestingly, a difference in composition between LCDs’ center and periphery is also hypothesized to be the reason why, on ICGA, LCDs appear with a characteristic “donut shape”, with a central hypercianescence bordered by a hypocianescent ring which, in turn, is itself surrounded by more hyper- and hypocianescent rings.
This correlates well with their appearance as shown on FAF, with a marked central hyperautofluorescence surrounded by a hypoautofluorescent halo, as well as en-face OCT, with a hyperreflective center bordered by a hyporeflective halo which, in turn, is surrounded by a hyper and a hypo-reflective ring.
LCDs have been classically described as associated with other early-onset drusen types, most frequently CDs; however, in our patient LCDs were found not to be associated with CDs or any other EOD types, consistently with what was observed by Sakurada et al. who proposed a distinction of CDs in three different subtypes, only the third of which was actually associated with Large Colloid Drusen.
LCDs were classically described as stable over time, with a low risk of vision-threatening complications. This was also confirmed by a recent report by Sassi et al. (2025), who provided a 10-year-long follow-up of LCDs with multimodal imaging. In this study, LCDs were proven to undergo dynamic remodeling over time, both through coalescing and spontaneously regressing, with a legacy of local retinal atrophy, which could either be represented by complete outer retinal atrophy, complete RPE and outer retinal atrophy, or incomplete RPE and outer retinal atrophy. However, retinal atrophy secondary to LCD regression was always limited in extension and only one case of GA was reported in the 10-year period; the same goes for MNVs secondary to LCD, with only one case reported in the study. LCDs have thus shown a favourable visual prognosis, which was confirmed in our patient as well.
The patient was recommended periodical routine checkups and evaluation with multimodal imaging.
Credit: Dr. Davide Sabbatino
Università degli Studi della Campania “Luigi Vanvitelli”
Instagram account: ataraxia_aponia
