
An 17 year-old female patient presented with a complaint of sudden visual decrease and central scotoma in both eyes, as well as progressive night vision deterioration over the past several years in both eyes. The patient’s visual acuities were 20/100 in the right eye and 20/80 in the left eye.
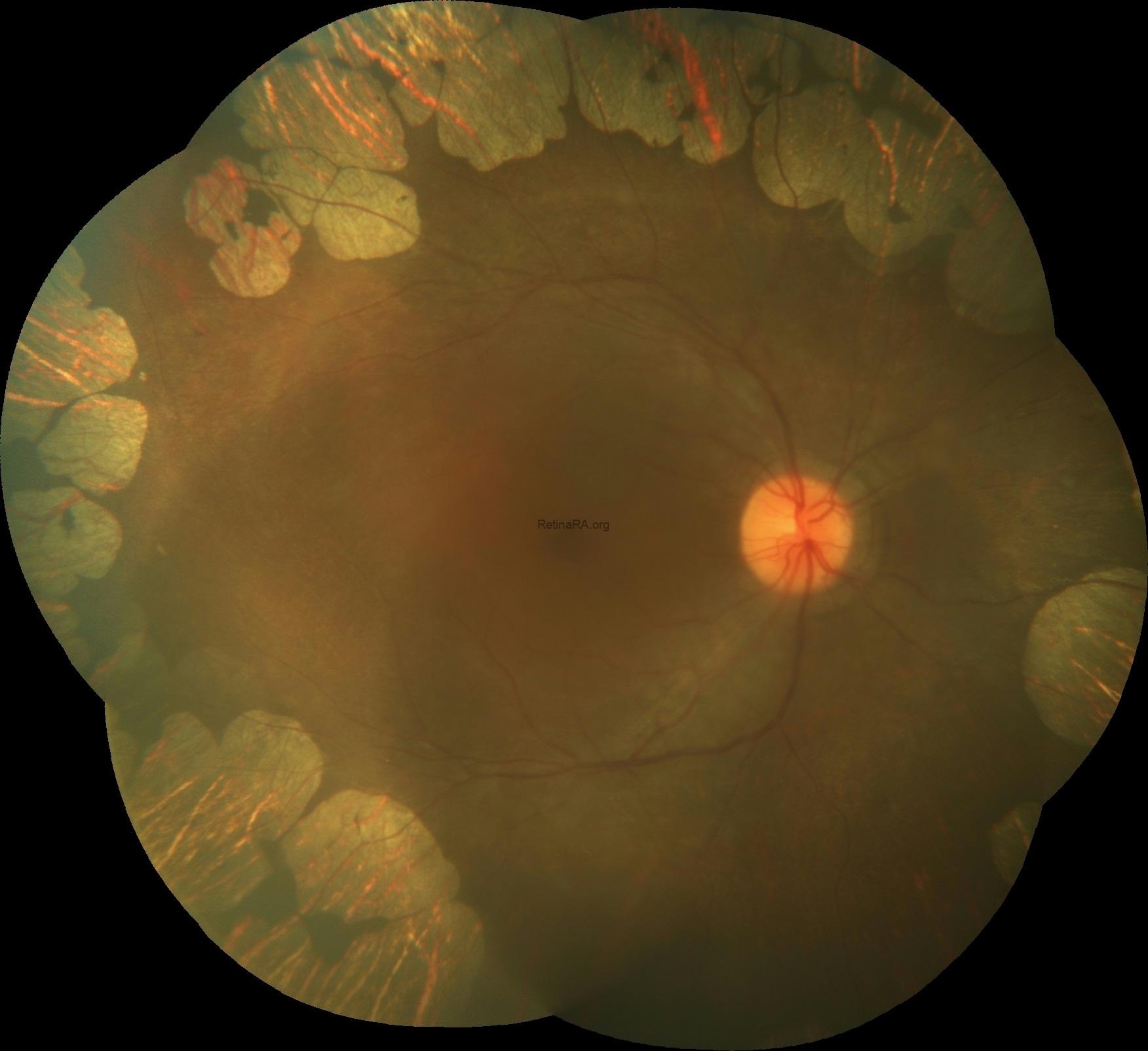

Moreover, an elevated level of plasma ornithine (967 Mmol/L) was detected, establishing the diagnosis of gyrate atrophy.
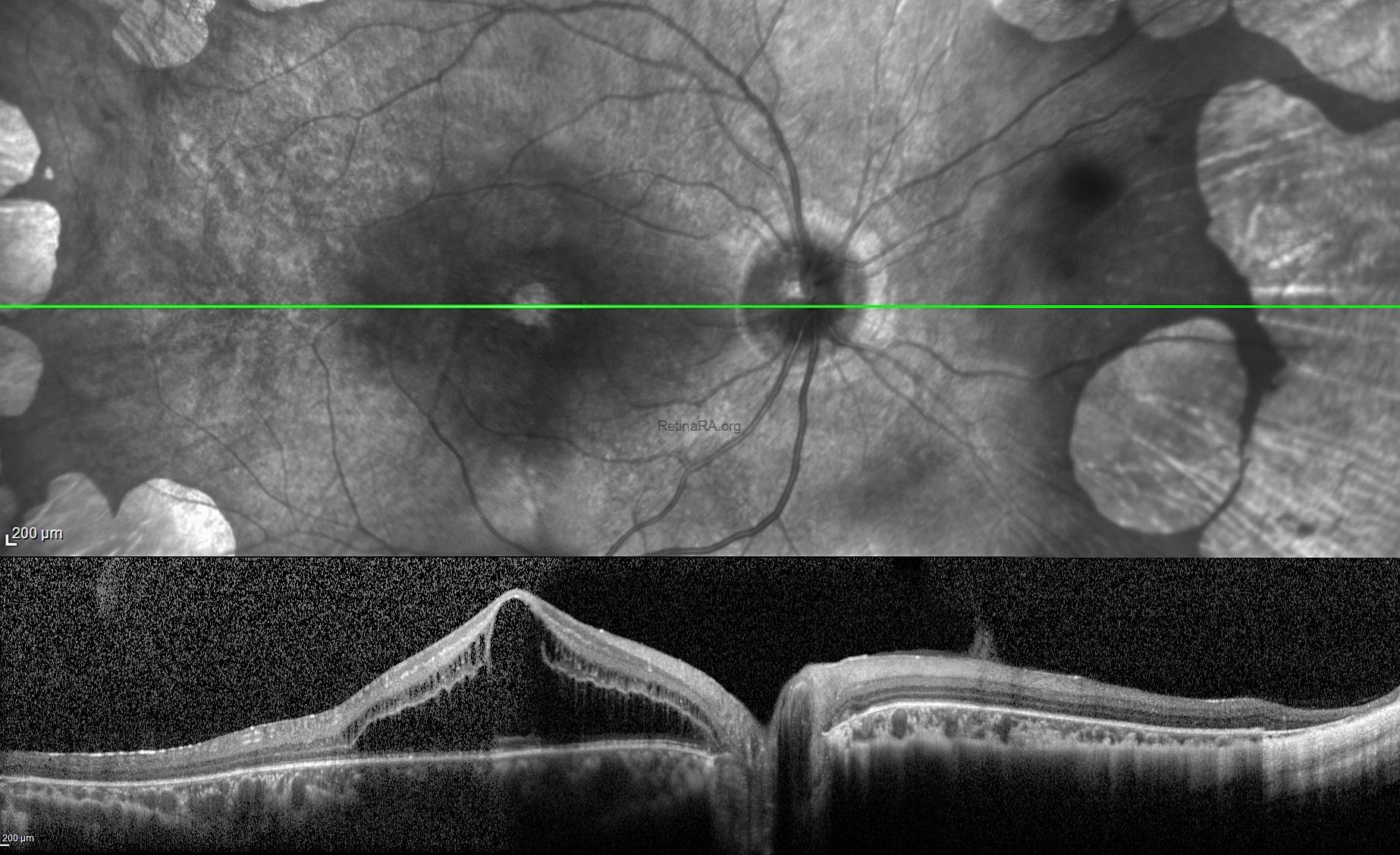
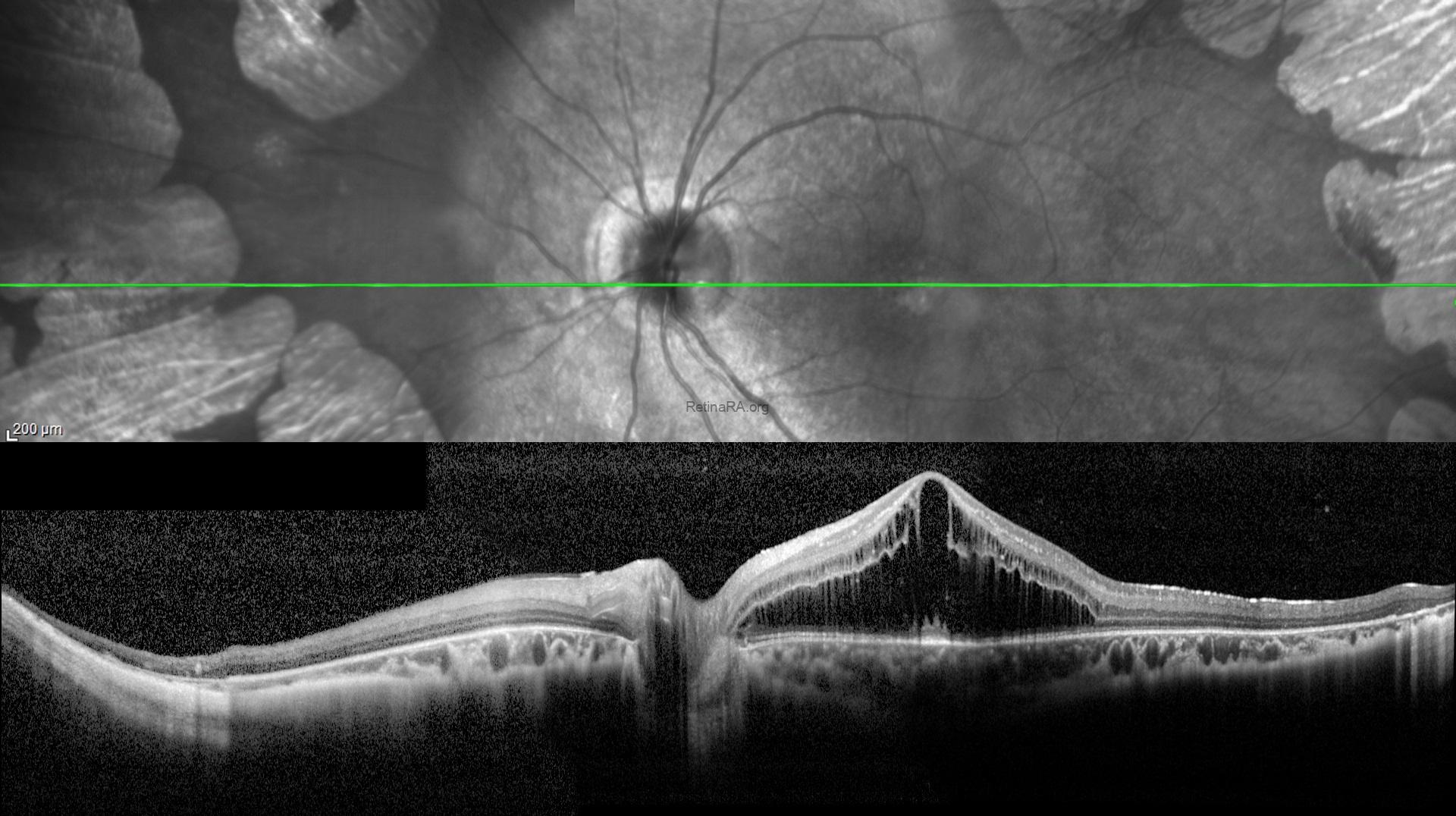
Gyrate atrophy of the choroid and retina is a rare, genetically determined, autosomal recessive metabolic disorder characterized by multiple sharply demarcated circular or oval areas of chorioretinal atrophy in the mid-periphery of the fundus which are initially separate and occur confluent with increasing age. A kind of macular involvement has been reported in this disease including cystoid macular edema, epimacular membrane, macular hole, and choroidal neovascularization. The foveoschisis refers to a splitting of the neurosensory retina, and is usually noted in highly myopic patients, Goldman-Favre Syndrome, and those with X-linked retinoschisis. However, the association of foveoschisis with gyrate atrophy is very rare. In this patient, examinations revealed no specific findings such as optic pits, myopic degeneration with staphyloma, or vitreoretinal traction, and we presume that the foveoschisis might have been triggered by gyrate atrophy.
Credit: Kemal Tekin, M.D., from Ulucanlar Eye Training and Research Hospital
Instagram accounts: @retina.academy and @dr.kemaltekin
