
A 16-year-old male patient presented with decreased vision in his right eye. Best-corrected visual acuity was 0.1 in the right eye and 1.0 in the left eye. Anterior segment examination was unremarkable in both eyes. Intraocular pressures were within normal range bilaterally.
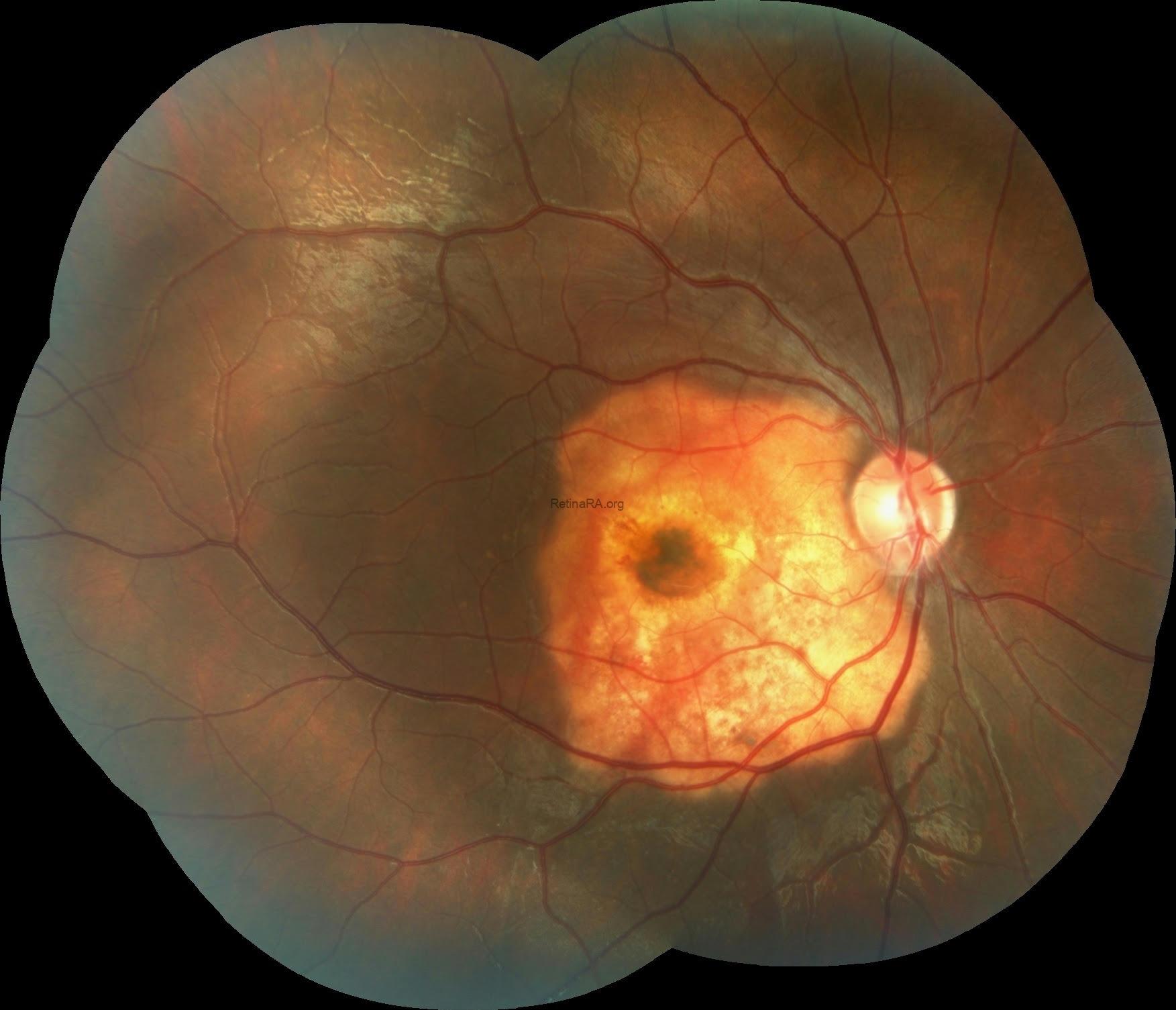
Fundus examination of the right eye revealed a well-circumscribed, elevated, yellow-orange lesion centered in the peripapillary and macular region in addition to foveal hemorrage while the left eye was completely normal. The lesion in the right eye has a geographic shape with irregular, scalloped borders and heterogeneous pigmentation. Central decalcification is suggested by the darker, atrophic area in the middle, while surrounding calcified regions exhibit a more solid, brighter orange tone. Retinal vessels are draped over the lesion without displacement, further supporting its subretinal/choroidal origin.
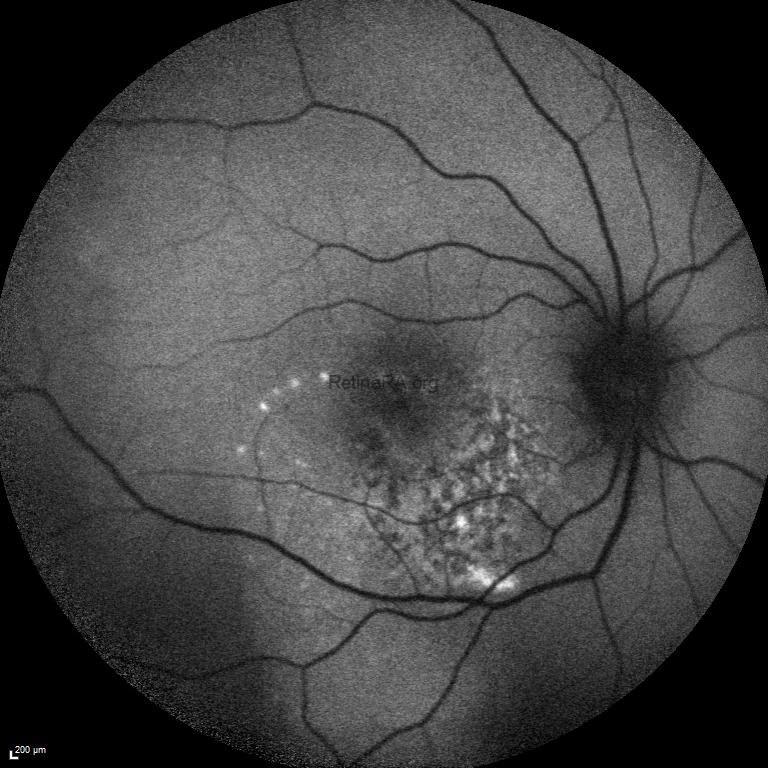
Fundus autofluorescence image demonstrated a mixed autofluorescence pattern. The central area appears hypoautofluorescent, suggestive of decalcification and retinal pigment epithelium atrophy. Surrounding this region, irregular zones of iso- to hyperautofluorescence reflect preserved or calcified segments of the lesion. The mottled autofluorescence is consistent with chronic remodeling of the lesion and may indicate areas at risk for functional deterioration.
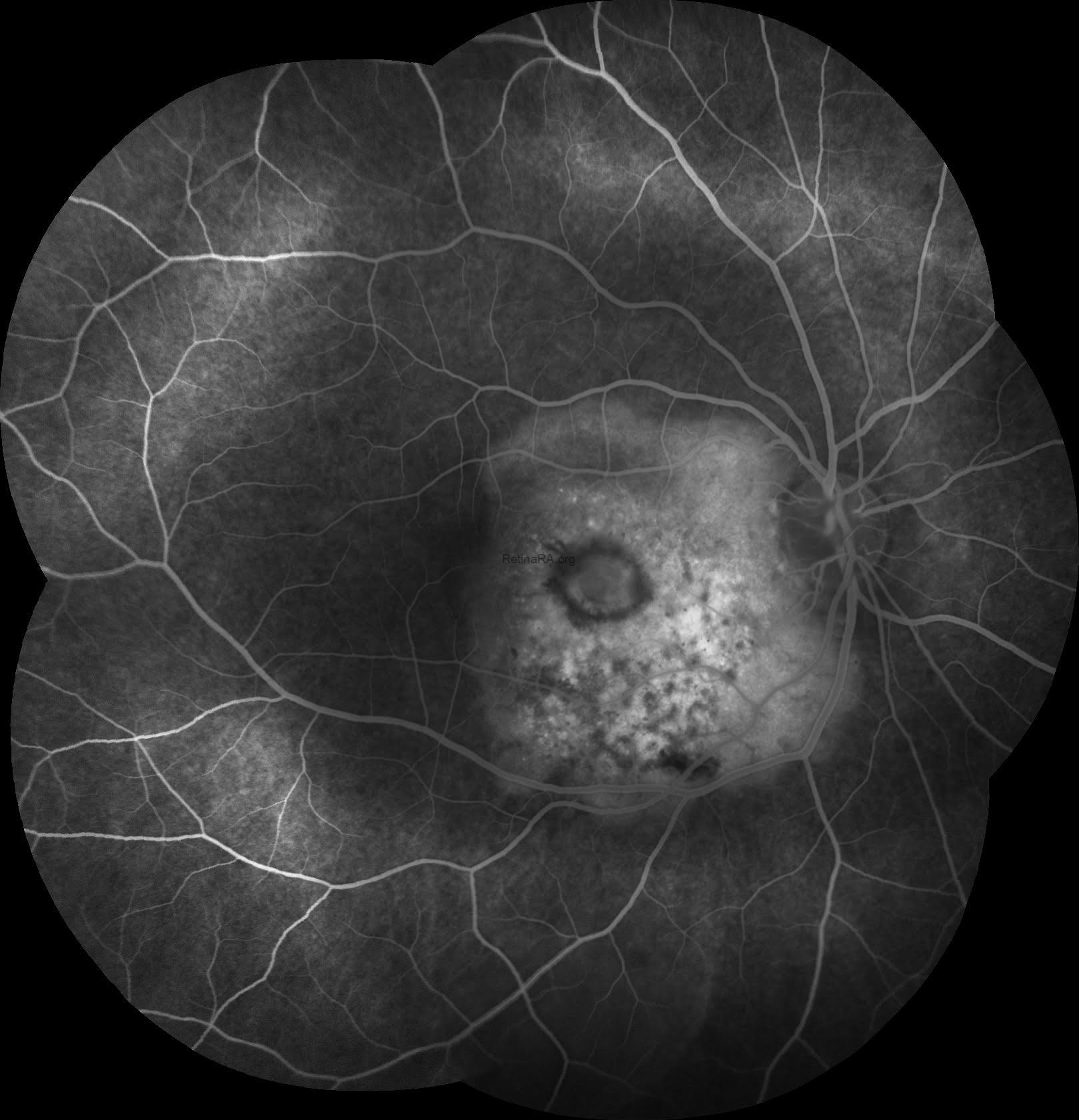
Fundus fluorescein angiography showed a mottled pattern of hyper- and hypofluorescence corresponding to the calcified and decalcified portions of the lesion. Early-phase images show background choroidal filling with blocked fluorescence in areas of dense calcification. The central dark ring suggests decalcification and possible RPE atrophy, while focal late hyperfluorescence may represent window defects or early choroidal neovascularization. The lesion borders remain relatively well demarcated throughout the angiographic sequence.
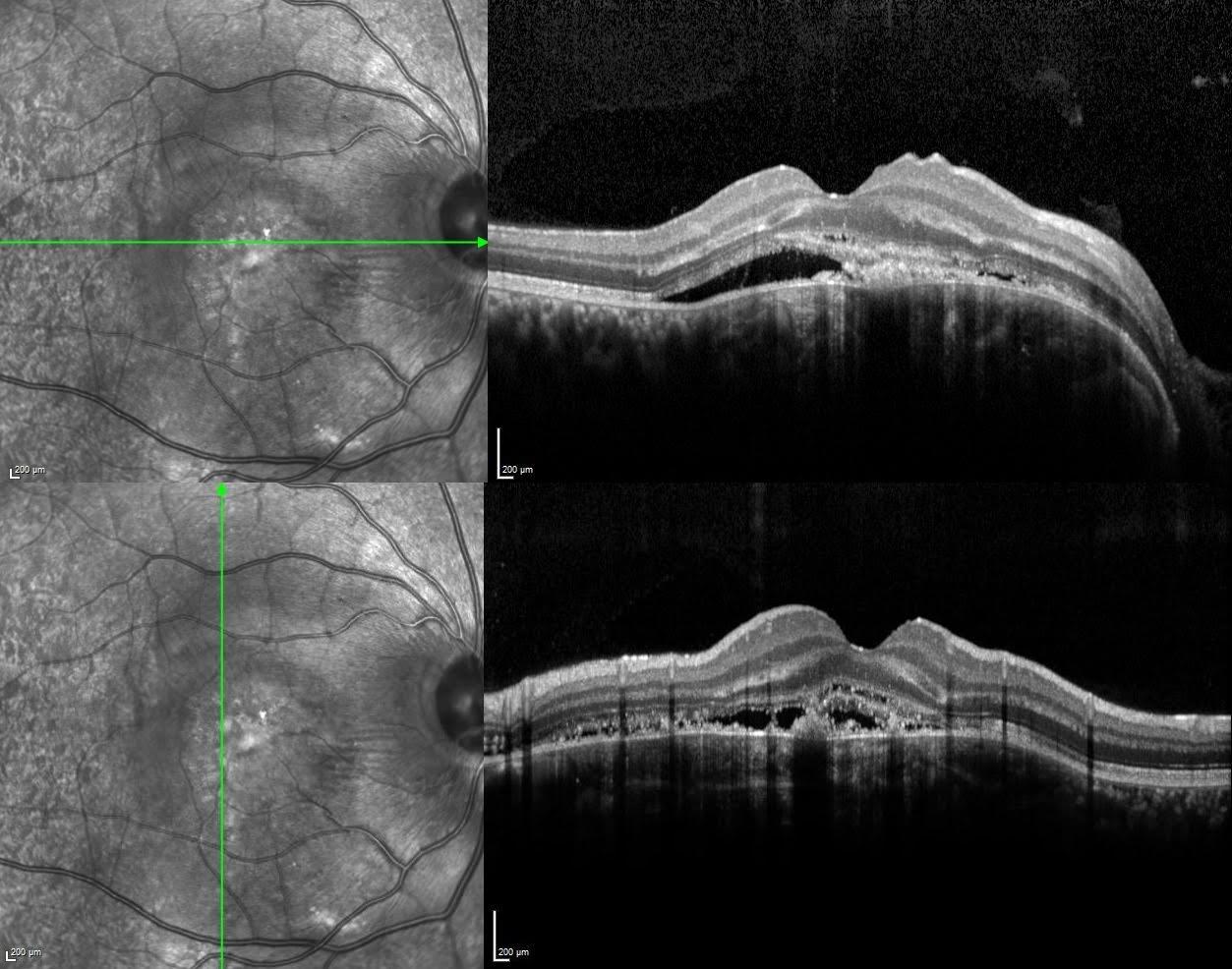
The OCT scan revealed a hyperreflective, plate-like choroidal lesion located beneath the RPE, consistent with choroidal osteoma. There is dense posterior shadowing due to the calcified mass, obscuring deeper structures. Overlying the lesion, the outer retinal layers exhibit thinning and disruption of the ellipsoid zone. A dome-shaped elevation of the RPE with underlying subretinal hyperreflective material suggests the presence of choroidal neovascularization, supported by intraretinal fluid and architectural distortion.
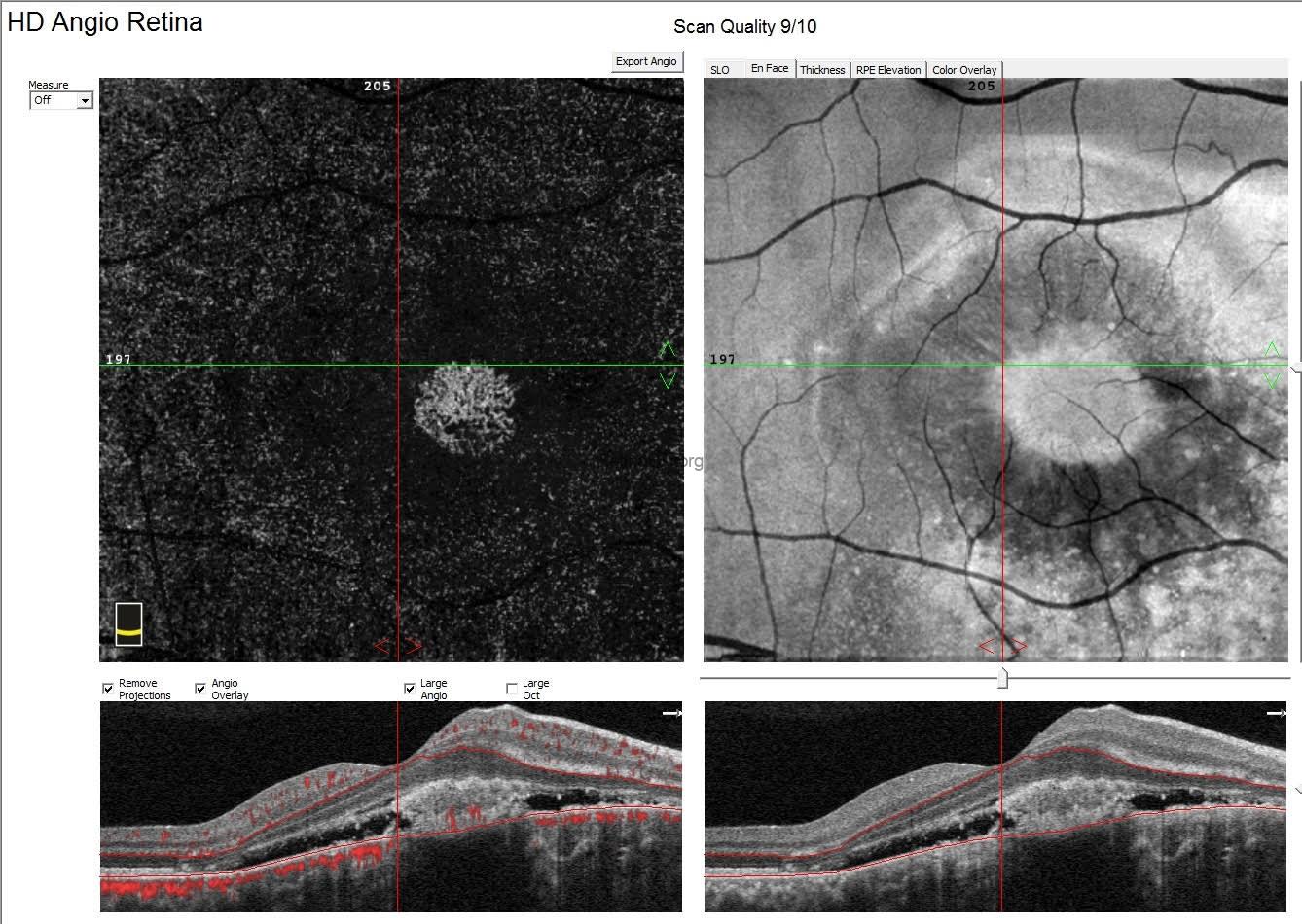
The OCTA image reveals flow voids in the area corresponding to the calcified portions of the choroidal osteoma, seen as hyporeflective regions due to signal attenuation. In the central macular region, irregular vascular networks are observed, suggesting secondary choroidal neovascularization (CNV). This HD-OCTA scan reveals a well-circumscribed, dense neovascular network within the outer retina or choriocapillaris layer, consistent with choroidal neovascularization (CNV) secondary to choroidal osteoma. The en face angiogram clearly shows a tangled vascular complex with high flow signal. Structural OCT demonstrates RPE elevation, subretinal hyperreflective material, and intraretinal fluid—all indicative of active CNV.
The axial orbital CT scan shows a hyperdense, plaque-like lesion located in the posterior aspect of the globe, along the choroid. The density of the lesion is comparable to cortical bone, confirming ossification typical of choroidal osteoma. The lesion does not appear to invade adjacent orbital structures or cause globe deformation. CT imaging is crucial for differentiating osteoma from other amelanotic intraocular lesions due to its ability to directly visualize calcification.

Choroidal osteoma is a rare, benign ossifying tumor of the choroid, typically affecting young healthy females in their second or third decade of life. It presents as a yellowish-white subretinal lesion, often located in the peripapillary or macular region. Though uncommon, it can be unilateral or bilateral. The exact pathogenesis remains unclear, but it is hypothesized to result from congenital hamartomatous differentiation or an acquired metaplastic process. Hormonal influences have also been suggested due to its female predominance. Patients may be asymptomatic or present with blurred vision, metamorphopsia, or scotomas, especially when the lesion involves the fovea. Visual decline can be progressive and is often associated with decalcification or complications such as choroidal neovascularization. Choroidal osteoma is a rare, benign ossifying tumor that arises within the choroid, most commonly affecting young women in their second or third decade of life. The lesion typically appears as a yellow-orange, well-demarcated subretinal mass, most often located near the optic disc or macula. Although the exact cause remains unclear, hormonal and congenital factors have been proposed. Many patients remain asymptomatic unless the lesion involves the fovea or complications such as choroidal neovascularization (CNV) develop.
Diagnosis relies on multimodal imaging. Fundus photography reveals the characteristic yellow-orange lesion, while OCT shows a hyperreflective plate-like mass beneath the RPE. FAF can differentiate calcified from decalcified areas, and ICGA typically shows persistent hypocyanescence. No treatment is needed for stable, asymptomatic lesions. However, if CNV occurs, intravitreal anti-VEGF therapy is the preferred option. Visual prognosis depends on lesion location and the presence of complications, necessitating regular follow-up.
and Sepideh Lotfi, MD
Biruni University School of Medicine, Department of Ophthalmology, Istanbul, Turkey
Instagram accounts: @sepidls