A 58-year-old woman presented with a sudden, painless decrease in vision in her left eye. Her medical history was notable for long-standing hypertension and hyperlipidemia. Best-corrected visual acuity was 20/20 in the right eye and 20/100 in the left eye. Anterior segment examination was unremarkable in both eyes, and intraocular pressures were within normal limits.
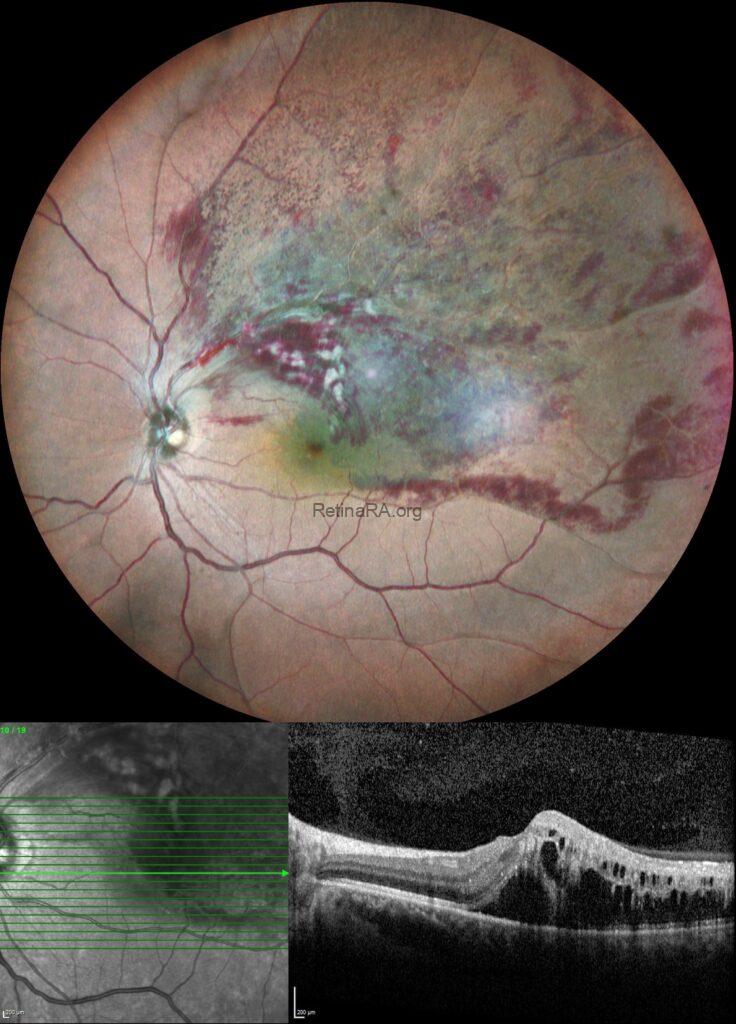
Color fundus photography of the left eye revealed sectoral flame-shaped and blot intraretinal hemorrhages confined to the superotemporal quadrant. Cotton-wool spots were present, and macular edema extending toward the fovea was noted.
 Color fundus photography of the right eye was unremarkable.
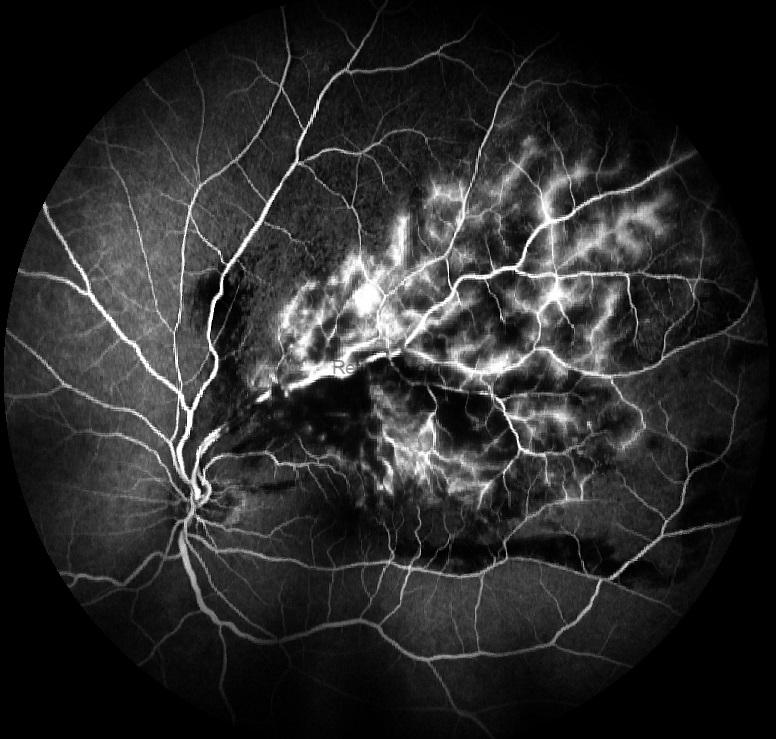
Color fundus photography of the right eye was unremarkable.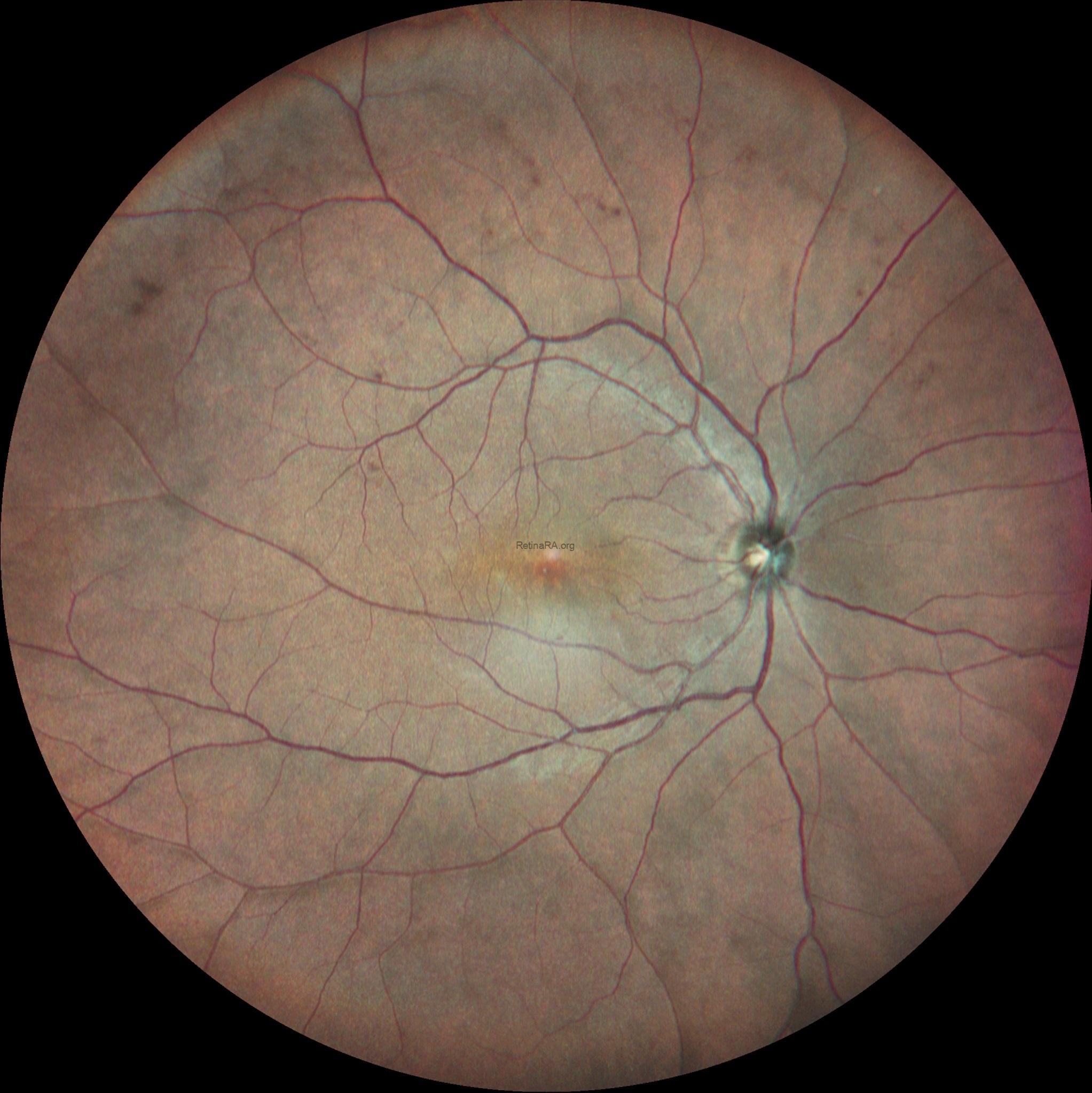 Fluorescein angiography of the left eye demonstrated delayed filling of the superotemporal retinal vein, blocked fluorescence corresponding to intraretinal hemorrhages, and late leakage from the retinal capillary bed.
Fluorescein angiography of the left eye demonstrated delayed filling of the superotemporal retinal vein, blocked fluorescence corresponding to intraretinal hemorrhages, and late leakage from the retinal capillary bed.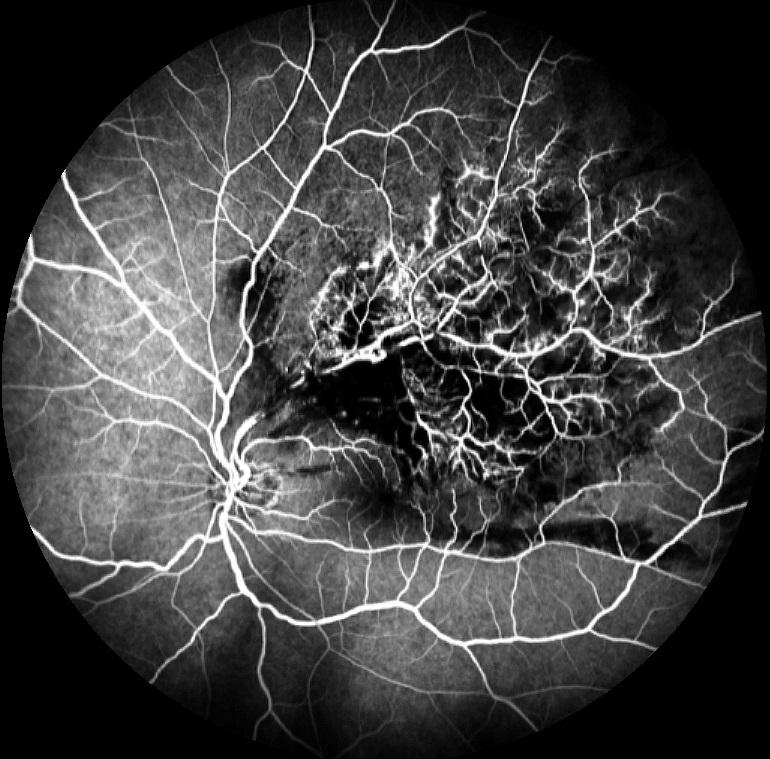
 Spectral-domain optical coherence tomography of the left eye showed increased central macular thickness with intraretinal cystoid spaces and subretinal fluid. Hyperreflective foci with posterior shadowing, consistent with hard exudates, were also observed.
Spectral-domain optical coherence tomography of the left eye showed increased central macular thickness with intraretinal cystoid spaces and subretinal fluid. Hyperreflective foci with posterior shadowing, consistent with hard exudates, were also observed. 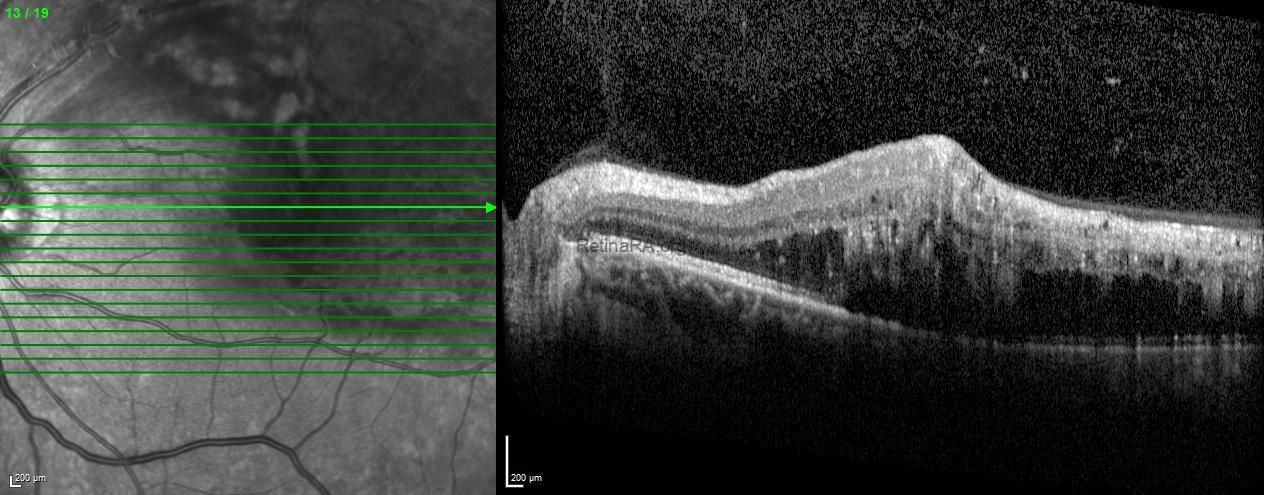
Based on the clinical and multimodal imaging findings, a diagnosis of superotemporal branch retinal vein occlusion with secondary macular edema was established. The patient was counseled regarding systemic risk factor control and scheduled for intravitreal anti–vascular endothelial growth factor (anti-VEGF) therapy, with close follow-up planned to monitor anatomical and visual outcomes.
Branch Retinal Vein Occlusion (BRVO) is the second most common retinal vascular disorder and typically occurs at arteriovenous crossings due to a shared adventitial sheath and compression of the retinal vein by a sclerotic arteriole. This leads to venous congestion, increased hydrostatic pressure, capillary damage, and disruption of the inner blood–retina barrier, resulting in intraretinal hemorrhage and macular edema. Multimodal imaging plays a critical role in diagnosis. Fluorescein angiography demonstrates delayed venous filling, capillary nonperfusion, and late phase leakage, while spectral-domain OCT reveals cystoid macular edema, subretinal fluid, and hyperreflective foci corresponding to lipid exudation. OCT angiography allows noninvasive visualization of superficial and deep capillary plexus alterations. Intravitreal anti-VEGF therapy is the current first-line treatment for BRVO-related macular edema.
Credit: Kemal Tekin, M.D., from Ulucanlar Eye Training and Research Hospital
Instagram accounts: @retina.academy and @dr.kemaltekin
