
A 15-year-old male patient complained of decreased vision in his left eye for a day. He was told by an ophthalmologist at another hospital that he should apply to a hospital with a pediatric neurologist, with a preliminary diagnosis of optic neuritis. He was admitted to our hospital by the Pediatric Neurology Department with a diagnosis of optic neuritis and an eye consultation was requested again. His visual acuity was 20/200 in the left eye. Anterior segment and vitreous examinations are unremarkable.
Color fundus photography shows optic nerve head swelling with an infiltrate at temporal margin. This infiltrate appears hyperfluorescent in early and late-phase fluorescein angiography.
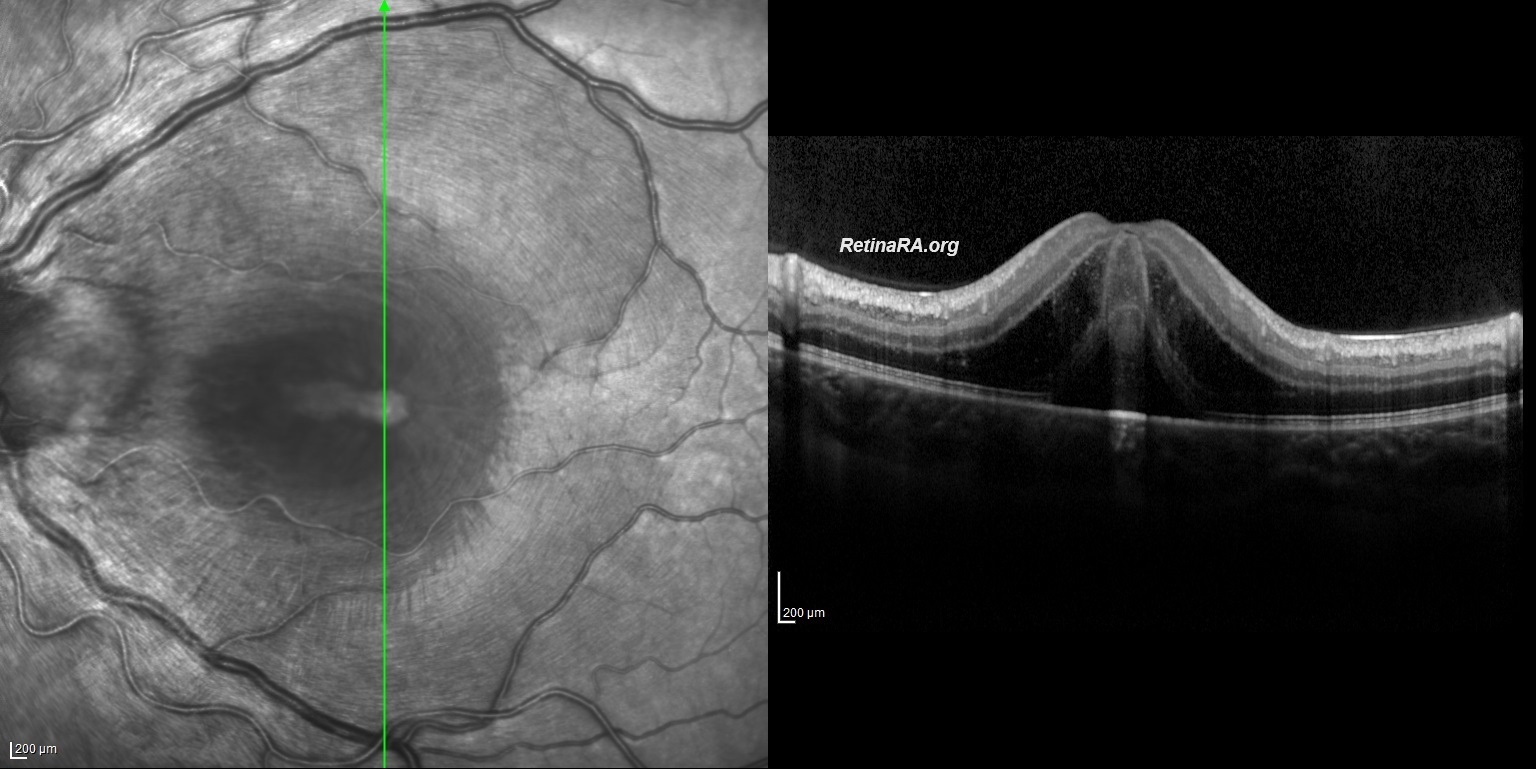
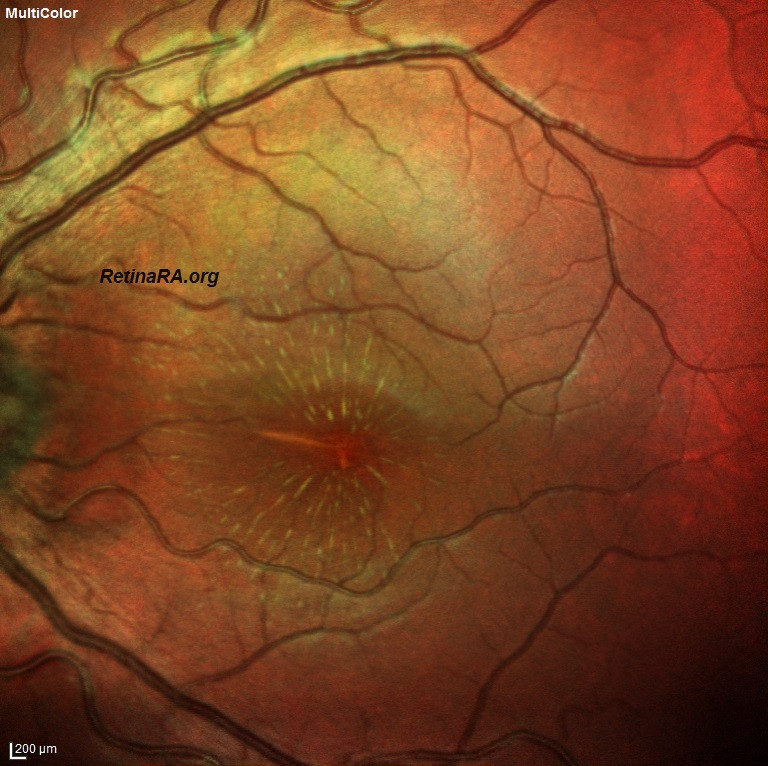
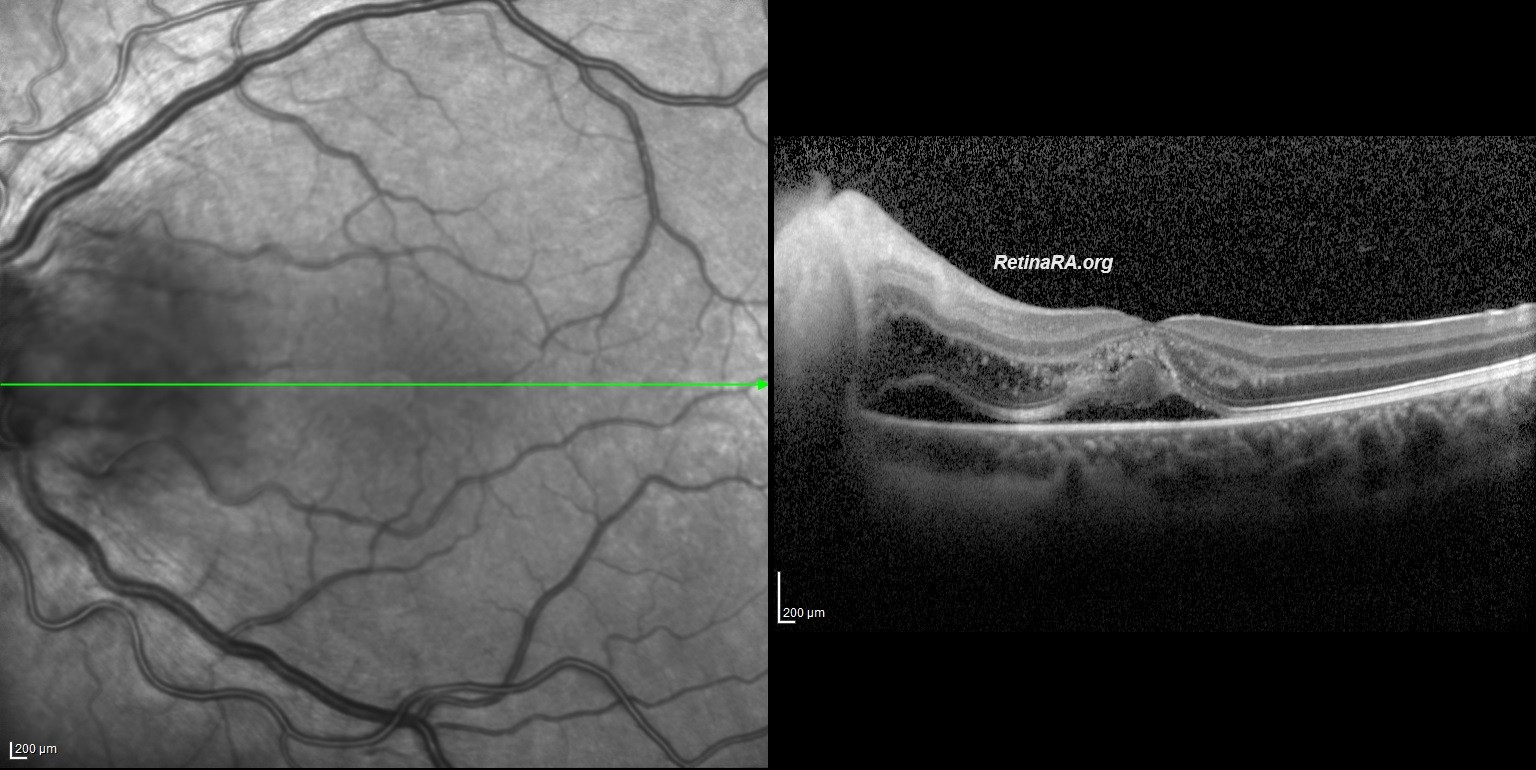
Macular edema was also present. The radial stretching lines seen in multicolor imaging and infrared reflectance imaging indicate fluid accumulation in Henle’s fiber layer. Vertical and horizontal OCT B-scans depict Macular edema with subretinal and intraretinal fluid. *Note that intraretinal fluid and exudate particularly accumulated in the Henle’s Fiber Layer. Neuroretinitis is characterized by an inflammation of the optic disc vasculature with exudation of fluid into the peripapillary retina. The lipid-rich component of the exudate is further able to penetrate into the Henle Fiber layer, creating what is clinically seen as a macular star pattern. Only the aqueous phase can pass through the external limiting membrane to accumulate beneath the neurosensory retina.
Differential Diagnosis
In patients presenting with optic disc edema and fluid accumulation in the subretinal region and Henle fiber layer, two diagnoses should first come to mind. One of these is malignant hypertensive retinopathy and the other is neuroretinitis. History of hypertension, bilaterality, and retinal hemorrhages support Malignant hypertensive retinopathy. Unilateral disease and infectious infiltration at the border of the optic disc and retina should suggest neuroretinitis. In both conditions, a macular star appearance may be present. The most common cause of neuroretinitis is Bartenolle Species, especially Hanselea. Other causes are Syphilis, Lyme disease, toxoplasmosis, toxocariasis, tuberculosis, histoplasmosis and leptospirosis.
Management
Bartonella Hanselea neuroretinitis was considered a preliminary diagnosis due to the history of being scratched by a cat 3 weeks ago. Empiric doxycycline and rifampicin were started. After the improvement seen on the 3rd day of antibiotic treatment and the negative results of Syphilis, toxocariasis and tuberculosis tests, 1 mg/kg methylprednisolone treatment was added to the patient. On the 9th day, Visual acuity improved to 20/30, healing continued and macular star appearance appeared. It is important to know that the macular star appearance in neuroretinitis occurs between the 7th and 10th days. The lipid-rich component of the exudate accumulated in the Henle fiber layer causes the appearance of the macular star. Some exudates settling on the outer retina, and ellipsoid zone alterations may also contribute to the macular star appearance.
The diagnosis of cat scratch disease was confirmed with Bartonella Henselae IgM+ results on the 20th day. Visual acuity increased to 20/25 and anatomical improvement continued.
Credit: M. Giray Ersoz, MD, FEBO
Biruni University School of Medicine, Department of Ophthalmology, Istanbul, Turkey
Instagram accounts: @retina.review and @retina.dr.girayersoz
1st-day imaging: Color fundus photography, multicolor imaging, fluorescein angiography, and OCT





9th-day imaging: Color fundus photography, multicolor imaging, and OCT

20th-day imaging: Color fundus photography, multicolor imaging, and OCT


